
-
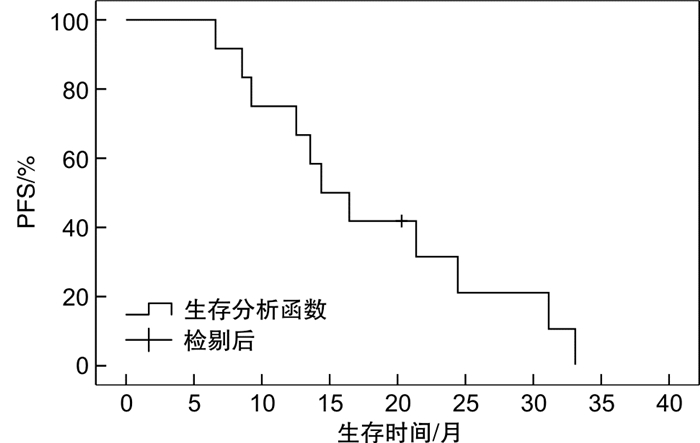
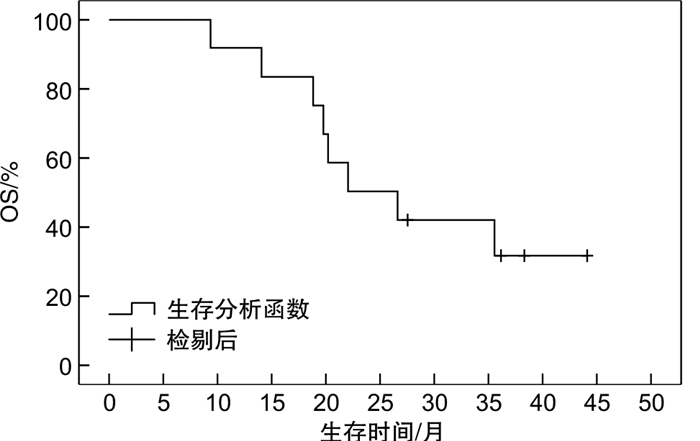
摘要: 目的 探讨原发性骨淋巴瘤(PBL)的临床特征及其对预后的影响。方法 对2014年12月—2019年12月收治的12例PBL患者资料进行回顾性分析,探讨其临床特征及预后影响因素。结果 12例患者病理类型均为弥漫大B细胞淋巴瘤,其中男5例,女7例;中位年龄59岁;主要发病部位为股骨(4例)和脊柱(3例);6例行放化疗联合治疗,6例行单纯化疗;全组患者中位随访时间为38.4个月,中位无进展生存时间为14.4(95%CI 9.5~19.3)个月,中位总生存时间为22.1(95%CI 11.1~33.1)个月。单因素分析结果显示,美国东部肿瘤研究组(ECOG)评分、有无软组织侵犯、初始治疗是否达完全缓解与总生存时间有关,β2微球蛋白水平、有无软组织侵犯与无进展生存时间有关(P<0.05)。而国际淋巴瘤预后指数(IPI)评分无论对于总生存时间还是无进展生存时间均差异无统计学意义。多因素分析结果提示,β2微球蛋白水平是影响患者无进展生存时间的独立预后因素(P<0.05)。结论 IPI对PBL患者预后的影响仍需进一步讨论,β2微球蛋白处于正常水平的PBL患者预后较好。可考虑根据β2微球蛋白水平,探讨针对PBL更合适的IPI评分模型。Abstract: Objective To investigate the clinical features and prognosis of primary bone lymphoma(PBL).Methods The clinical data of 12 patients with PBL from December 2014 to December 2019 were retrospectively analyzed to explore the clinical characteristics and prognostic factors.Results The pathological type of 12 patients was diffuse large B-cell lymphoma, including 5 males and 7 females, with a median age of 59 years old. The main sites were femur(4 cases) and spine(3 cases). Six patients received combined radiotherapy and chemotherapy, and 6 patients received chemotherapy alone. The median follow-up time was 38.4 months, the median progression-free survival was 14.4(95%CI 9.5-19.3) months, and the median overall survival was 22.1(95%CI 11.1-33.1) months. Univariate analysis showed that ECOG score, presence or absence of soft tissue invasion and initial treatment of complete remission were associated with overall survival, while β2 microglobulin level and the presence or absence of soft tissue invasion were associated with progression-free survival(P < 0.05). IPI score has no statistical significance for overall survival or progression-free survival. Multivariate analysis indicated that β2 microglobulin level was an independent prognostic factor of progression-free survival(P < 0.05).Conclusion The influence of IPI on the prognosis of PBL patients still needs further discussion. The prognosis of PBL patients with normal β2 microglobulin levels is better. A more appropriate IPI scoring model could be explored based on the level of β2 microglobulin.
-
Key words:
- primary bone lymphoma /
- clinical features /
- prognosis
-

-
表 1 影响12例PBL患者预后的单因素分析
影响因素 例数 OS/月 PFS/月 中位值(95%CI) P 中位值(95%CI) P 性别 0.320 0.437 男 5 35.6(6.6~64.6) 14.4(12.7~16.1) 女 7 19.8(17.5~22.1) 16.5(6.5~26.5) 年龄/岁 0.840 0.576 ≥60 6 22.1(12.7~31.5) 13.6(11.4~15.8) <60 6 20.2(1.2~39.2) 16.5(4.2~28.8) 分子亚型 0.298 0.372 GCB 7 19.8(17.5~22.1) 24.5(11.3~37.7) non-GCB 5 35.6(21.7~49.5) 13.6(11.0~16.2) 骨病变数量 0.294 0.388 单个 6 未达到 14.4(6.9~21.9) 多个 6 19.8(16.0~23.6) 9.2(0~18.7) 分期 0.416 0.974 ⅠE+ⅡE期 7 36.6(4.0~67.2) 14.4(12.3~16.5) Ⅳ期 5 22.1(15.2~29.0) 16.5(0~33.5) ECOG评分 0.003 0.073 ≤2 7 未达到 24.5(3.8~45.2) >2 5 18.9(8.6~29.2) 12.6(5.3~19.9) 周围软组织侵犯 0.001 0.003 无 6 18.9(12.1~25.7) 24.5(18.0~31.0) 有 6 未达到 9.2(4.4~14.0) IPI评分 0.892 0.379 ≤2 6 20.2(1.2~39.2) 14.4(0~32.8) >2 6 22.1(12.7~31.5) 13.6(9.0~18.3) LDH/(U·L-1) 0.246 0.662 <240 4 未达到 13.6(1.1~26.1) ≥240 8 19.8(18.0~21.6) 14.4(9.0~19.8) β2微球蛋白 0.243 0.004 正常 7 35.6(17.3~53.9) 24.5(15.8~33.2) 升高 5 20.2(7.1~33.3) 12.6(4.0~21.2) 联合放疗 0.983 0.768 有 6 20.2(5.0~35.4) 13.6(11.4~15.8) 无 6 22.1(12.7~31.5) 16.5(1.1~31.9) 初始CR 0.027 0.086 否 5 19.8(17.9~21.7) 12.6(5.3~19.9) 是 7 未达到 24.5(3.8~45.2) 利妥昔单抗 0.903 0.135 未使用 6 22.1(13.8~30.4) 12.6(7.3~17.9) 使用 6 20.2(4.2~36.2) 16.5(0.4~32.6)  下载: 导出CSV
下载: 导出CSV
表 2 影响12例PBL患者PFS的Cox多因素分析
影响因素 β SE Wald χ2 HR 95%CI P β2微球蛋白 -2.677 1.333 4.036 0.069 0.005~0.937 0.045 ECOG评分 -1.227 1.468 0.699 0.293 0.016~5.206 0.403 软组织侵犯 -1.177 1.250 0.887 0.308 0.027~3.571 0.887 初始反应 0.350 1.481 0.056 1.419 0.078~25.878 0.813
下载: 导出CSV
-
[1] 王小桐, 夏秋媛, 贺慧颖, 等. 新近认识的软组织肿瘤命名和分类的思考[J]. 中华病理学杂志, 2021, 50(5): 442-446. doi: 10.3760/cma.j.cn112151-20200802-00614
[2] Choi JH, Ro JY. The 2020 WHO Classification of Tumors of Bone: An Updated Review[J]. Adv Anat Pathol, 2021, 28(3): 119-138. doi: 10.1097/PAP.0000000000000293
[3] Kim SY, Shin DY, Lee SS, et al. Clinical characteristics and outcomes of primary bone lymphoma in Korea[J]. Korean J Hematol, 2012, 47(3): 213-218. doi: 10.5045/kjh.2012.47.3.213
[4] Liu CX, Xu TQ, Xu L, et al. Primary lymphoma of bone: a population-based study of 2558 patients[J]. Ther Adv Hematol, 2020, 11: 2040620720958538.
[5] Bindal P, Desai A, Delasos L, et al. Primary Bone Lymphoma: A Case Series and Review of Literature[J]. Case Rep Hematol, 2020, 2020: 4254803.
[6] Tazi I, Benmoussa A, Boufarissi FZ, et al. Les lymphomes non-Hodgkiniens osseux de l'adulte[Adult non-Hodgkin bone lymphomas][J]. Bull Cancer, 2021, 108(4): 424-434. doi: 10.1016/j.bulcan.2020.12.010
[7] 陈琪, 赵冰冰, 赵维莅, 等. 原发和继发骨淋巴瘤患者的临床特征和预后分析[J]. 临床血液学杂志, 2017, 30(11): 853-855, 858. doi: 10.13201/j.issn.1004-2806.2017.11.009 http://lcxz.cbpt.cnki.net/WKC/WebPublication/paperDigest.aspx?paperID=b41c896d-39bc-4591-aa7f-c354346b65ec
[8] 李元吉, 李玉富, 杜建伟, 等. 11例原发性骨淋巴瘤临床分析[J]. 中华血液学杂志, 2017, 38(7): 597-601. https://www.cnki.com.cn/Article/CJFDTOTAL-DYJD201303030.htm
[9] Govi S, Christie D, Mappa S, et al. The clinical features, management and prognosis of primary and secondary indolent lymphoma of the bone: a retrospective study of the International Extranodal Lymphoma Study Group(IELSG #14 study)[J]. Leuk Lymphoma, 2014, 55(8): 1796-1799. doi: 10.3109/10428194.2013.853298
[10] Steffner RJ, Jang ES, Danford NC. Lymphoma of Bone[J]. JBJS Rev, 2018, 6(1): e1. doi: 10.2106/JBJS.RVW.17.00006
[11] Sharma A, Ahmed R, Agrawal N, et al. Primary Bone Lymphoma: A 13 Year Retrospective Institutional Analysis in the Chemo-Immunotherapy Era[J]. Indian J Hematol Blood Transfus, 2021, 37(2): 240-248. doi: 10.1007/s12288-020-01327-3
[12] Alencar A, Pitcher D, Byrne G, et al. Primary bone lymphoma-the University of Miami experience[J]. Leuk Lymphoma, 2010, 51(1): 39-49. doi: 10.3109/10428190903308007
[13] Kazama H, Teramura M, Yoshinaga K, et al. Long-term remission of primary bone marrow diffuse large B-cell lymphoma treated with high-dose chemotherapy rescued by in vivo rituximab-purged autologous stem cells[J]. Case Rep Med, 2012, 2012: 957063.
[14] Müller A, Dreyling M, Roeder F, et al. Primary bone lymphoma: Clinical presentation and therapeutic considerations[J]. J Bone Oncol, 2020, 25: 100326. doi: 10.1016/j.jbo.2020.100326
[15] Santos T, Zumárraga JP, Reaes FM, et al. Primary bone lymphomas: retrospective analysis of 42 consecutive cases[J]. Acta Ortop Bras, 2018, 26(2): 103-107. doi: 10.1590/1413-785220182602185549
[16] Barbieri E, Cammelli S, Mauro F, et al. Primary non-Hodgkin's lymphoma of the bone: treatment and analysis of prognostic factors for Stage Ⅰ and Stage Ⅱ[J]. Int J Radiat Oncol Biol Phys, 2004, 59(3): 760-764. doi: 10.1016/j.ijrobp.2003.11.020
[17] Mahmood H, Habib M, Aslam W, et al. Clinicopathological spectrum of diffuse large B cell lymphoma: a study targeting population yet unexplored in Pakistan[J]. BMC Res Notes, 2021, 14(1): 354. doi: 10.1186/s13104-021-05768-5
[18] Ayesh Haj Yousef MH, Audat Z, Al-Shorafat DM, et al. Primary Diffuse Large B Cell Lymphoma of Bone: A Single-Center Experience[J]. J Blood Med, 2022, 13: 143-149. doi: 10.2147/JBM.S350655
[19] Li X, Xu-Monette ZY, Yi S, et al. Primary Bone Lymphoma Exhibits a Favorable Prognosis and Distinct Gene Expression Signatures Resembling Diffuse Large B-Cell Lymphoma Derived From Centrocytes in the Germinal Center[J]. Am J Surg Pathol, 2017, 41(10): 1309-1321. doi: 10.1097/PAS.0000000000000923
[20] 邹夏, 李妮, 万阳阳, 等. NHL患者血清LDH、β2-MG及CD44水平与病情和预后的关系[J]. 西部医学, 2021, 33(6): 856-859. doi: 10.3969/j.issn.1672-3511.2021.06.015
[21] 黄天骄, 周虹, 刘松涛, 等. 弥漫大B细胞淋巴瘤患者血清中乳酸脱氢酶、β2微球蛋白及尿酸临床意义[J]. 临床血液学杂志, 2021, 34(6): 412-414. doi: 10.13201/j.issn.1004-2806.2021.06.008 http://lcxz.cbpt.cnki.net/WKC/WebPublication/paperDigest.aspx?paperID=5ab5012c-4fa7-4c53-86d1-681b918570ca
[22] Milanovic N, Matkovic S, Ristic D, et al. Significance of tumor burden, vascular endothelial growth factor, lactate dehydrogenase and beta-2 microglobulin serum levels in advanced diffuse large B cell lymphoma[J]. J BUON, 2012, 17(3): 497-501.
[23] 仲凯励, 曹宝平, 郭晓川, 等. 初治原发性骨淋巴瘤患者的临床特征和长期预后分析[J]. 中国实验血液学杂志, 2022, 30(1): 126-130. doi: 10.19746/j.cnki.issn1009-2137.2022.01.020
-
图(2)
表(2)
计量
- 文章访问数: 960
- PDF下载数: 89
- 施引文献: 0