
Comparison of 18F-FDG PET/CT and bone marrow biopsy in detection of bone marrow involvement in diffuse large B-cell lymphoma
-
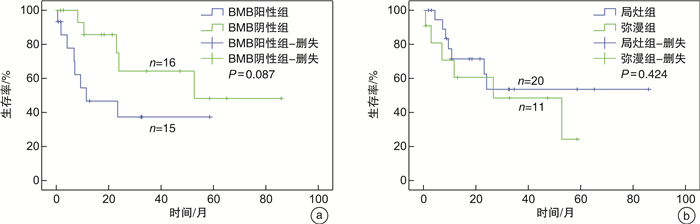
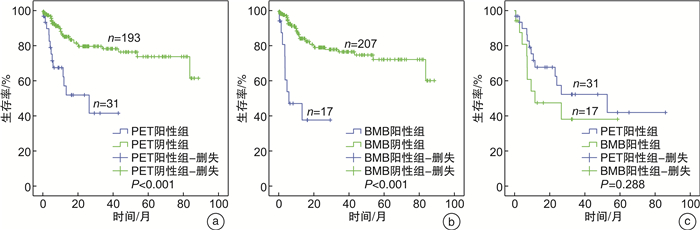
摘要: 目的 评估18F-FDG PET/CT与骨髓活检(BMB)对弥漫性大B细胞淋巴瘤(DLBCL)患者骨髓浸润(BMI)的诊断效能,明确PET/CT能否替代BMB成为BMI的诊断手段。方法 回顾性分析2014年1月—2022年4月初诊的224例DLBCL患者,所有患者化疗前均接受PET/CT和BMB检查。比较PET/CT与BMB诊断BMI的敏感度、特异度、阳性预测值、阴性预测值、漏诊率、2种方法的一致性、对分期的影响,比较PET阳性患者中BMB阳性组与BMB阴性组、局灶组与弥漫组血常规、乳酸脱氢酶(LDH)、总生存期(OS)的差别。结果 224例患者中共检出BMI阳性患者33例(14.7%),其中PET/CT检出31例(13.8%),BMB检出17例(7.6%)。PET/CT与BMB检出BMI的敏感度分别为93.9%、51.5%,特异度分别为100.0%、100.0%,阳性预测值分别为100.0%、100.0%,阴性预测值分别为99.0%、92.3%,漏诊率分别为6.1%、48.5%。PET/CT与BMB诊断一致的206例(92.0%),包括191例均阴性,15例均阳性。诊断不一致的18例(8.0%),包括PET阳性BMB阴性16例,PET阴性BMB阳性2例。PET/CT将3例患者由Ⅲ期升级为Ⅳ期,BMB将1例患者由Ⅲ期升级为Ⅳ期。PET阳性患者中,BMB阳性组与BMB阴性组白细胞、中性粒细胞、淋巴细胞、血红蛋白、血小板计数差异无统计学意义(P>0.05),BMB阳性组LDH高于BMB阴性组(P=0.031)。31例PET阳性患者中局灶组20例、弥漫组11例。弥漫组BMB阳性比例明显高于局灶组(81.8% vs 30.0%,P=0.009)。弥漫组血小板计数低于局灶组(P=0.004)。所有患者PET阳性组较PET阴性组、BMB阳性组较BMB阴性组OS均显著缩短(P < 0.001)。PET阳性与BMB阳性患者OS差异无统计学意义(P=0.288)。PET阳性患者中BMB阳性组与BMB阴性组中位OS分别为5.8个月、26.4个月,1年OS率分别为(37.3±13.9)%、(64.3±14.9)%(P=0.087)。局灶组与弥漫组OS差异无统计学意义(P=0.424)。结论 PET/CT评估BMI较BMB诊断效能高,PET/CT与BMB诊断的BMI均具有预后意义。PET阳性患者中BMB状态可能存在预后价值。DLBCL患者可首先行PET/CT,PET阴性者可考虑取消BMB,PET阳性者建议进一步行BMB,可在今后研究中进一步探讨其必要性。
-
关键词:
- 弥漫性大B细胞淋巴瘤 /
- 18F-FDG PET/CT /
- 骨髓活检 /
- 骨髓浸润
Abstract: Objective To evaluate the role of fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography(18F-FDG PET/CT) and bone marrow biopsy(BMB) in detecting bone marrow involvement(BMI) in diffuse large B-cell lymphoma(DLBCL) and then determine whether PET/CT could replace BMB for the assessment of BMI.Methods This is a retrospective analysis of 224 newly diagnosed DLBCL patients who presented to our hospital during January 2014 and April 2022 who received concurrent PET/CT and BMB examination before chemotherapy. Sensitivity, specificity, positive predictive value, negative predictive value and omission diagnostic rate were compared between PET/CT and BMB. Concordance of both techniques and their influences on DLBCL staging were analyzed. In PET-positive patients, blood routine examination, lactate dehydrogenase(LDH) level and overall survival(OS) were compared between BMB-positive and BMB-negative groups as well as focal and diffuse involvement groups.Results In a total of 33 BMI cases (14.7%), 31 cases (13.8%) was detected by PET/CT and 17 cases(7.6%) by BMB. For PET/CT and BMB, sensitivity was 93.9% and 51.5%, specificity 100.0% and 100.0%, positive predictive value 100.0% and 100.0%, negative predictive value 99.0% and 92.3%, omission diagnostic rate 6.1% and 48.5%, respectively. Two hundred and six(92%) patients had concordant results between PET/CT and BMB(191 patients were negative for both, 15 patients were positive for both). Eighteen(8.0%) patients had a discordant interpretation(16 patients were negative by BMB and positive by PET/CT and 2 patients were positive by BMB and negative by PET/CT). Three patients were upstaged from stage Ⅲ to Ⅳ by PET/CT and one patient was upstaged from stage Ⅲ to Ⅳ by BMB. For PET-positive patients, there was no difference in white blood cell, neutrocyte, lymphocyte, hemoglobin and platelet between BMB-positive subgroup and BMB-negative subgroup(P>0.05) while LDH was higher in BMB-positive subgroup than BMB-negative subgroup(P=0.031). Among 31 PET-positive cases, 20 cases had focal(1 unifocal and 19 multifocal) while 11 cases had diffuse involvement. Patients with diffuse involvement had a larger proportion of positive BMB compared with focal involvement cases(81.8% vs 30.0%, P=0.009). Platelet was lower in diffuse involvement patients than focal involvement ones(P=0.004). Among all of 224 patients, PET-positive and BMB-positive cases had worse OS than PET-negative and BMB-negative cases respectively(P < 0.001). There was no difference on OS between PET-positive and BMB-positive cases(P=0.288). In PET-positive patients, median OS was 5.8 months, 26.4 months and 1-year OS probability was(37.3±13.9)%, (64.3±14.9)% for BMB-positive and BMB-negative subgroup respectively(P=0.087). OS was not different between focal and diffuse involvement patients(P=0.424).Conclusion PET/CT showed superior performance in detecting BMI than BMB in DLBCL. Both PET/CT and BMB defined BMI had prognostic values. BMB might had a prognostic value in PET-positive patients. For DLBCL patients, bone marrow status can be assessed firstly by means of PET/CT; in negative cases BMB could be omitted and in positive cases BMB is recommended to be carried out afterwards, which needs further verification. -

-
表 1 PET阳性患者中BMB阳性组与BMB阴性组血常规、LDH的比较
X±S 组别 WBC/(×109/L) 中性粒细胞/(×109/L) 淋巴细胞/(×109/L) HGB/(g/L) PLT/(×109/L) LDH/(U/L) BMB阳性(n=15) 7.73±4.65 4.34±2.38 2.32±2.82 123.60±21.99 154.93±125.33 1 050.07±856.32 BMB阴性(n=16) 5.51±1.86 3.78±1.50 1.08±0.55 115.75±21.72 213.31±103.14 498.19±332.06 F 5.911 3.842 3.908 0.012 1.085 6.457 P 0.103 0.440 0.093 0.326 0.166 0.031  下载: 导出CSV
下载: 导出CSV
表 2 PET阳性患者中局灶组与弥漫组血常规、LDH的比较
X±S 组别 WBC/(×109/L) 中性粒细胞/(×109/L) 淋巴细胞/(×109/L) HGB/(g/L) PLT/(×109/L) LDH/(U/L) 局灶组(n=20) 5.80±1.86 3.78±1.53 1.27±0.74 121.90±20.70 227.35±120.13 554.30±373.76 弥漫组(n=11) 8.01±5.40 4.54±2.59 2.43±3.29 115.27±24.24 108.18±55.58 1 148.73±954.78 F 10.998 4.703 5.274 2.336 2.702 6.969 P 0.214 0.389 0.274 0.428 0.004 0.071
下载: 导出CSV
-
[1] Kaddu-Mulindwa D, Altmann B, Held G, et al. FDG PET/CT to detect bone marrow involvement in the initial staging of patients with aggressive non-Hodgkin lymphoma: results from the prospective, multicenter PETAL and OPTIMAL>60 trials[J]. Eur J Nucl Med Mol Imaging, 2021, 48(11): 3550-3559. doi: 10.1007/s00259-021-05348-6
[2] 谢萌, 张青青, 郭瑞昕, 等. 头颈部弥漫性大B细胞淋巴瘤的临床特征分析[J]. 临床耳鼻咽喉头颈外科杂志, 2022, 36(1): 1-7. https://www.cnki.com.cn/Article/CJFDTOTAL-LCEH202201001.htm
[3] Kandeel AA, Hussein M, Zidan L, et al. Diagnostic performance of 18F-2-fluoro-2-deoxy-D-glucose PET/computerized tomography in identifying bone marrow infiltration in new patients with diffuse large B-cell lymphoma and Hodgkin lymphoma[J]. Nucl Med Commun, 2020, 41(3): 269-279. doi: 10.1097/MNM.0000000000001139
[4] Nakajima R, Moskowitz AJ, Michaud L, et al. Baseline FDG-PET/CT detects bone marrow involvement in follicular lymphoma and provides relevant prognostic information[J]. Blood Adv, 2020, 4(8): 1812-1823. doi: 10.1182/bloodadvances.2020001579
[5] Han EJ, O JH, Yoon H, et al. Comparison of FDG PET/CT and Bone Marrow Biopsy Results in Patients with Diffuse Large B Cell Lymphoma with Subgroup Analysis of PET Radiomics[J]. Diagnostics(Basel), 2022, 12(1): 222.
[6] El Karak F, Bou-Orm IR, Ghosn M, et al. PET/CT Scanner and Bone Marrow Biopsy in Detection of Bone Marrow Involvement in Diffuse Large B-Cell Lymphoma[J]. PLoS One, 2017, 12(1): e0170299. doi: 10.1371/journal.pone.0170299
[7] Al-Sabbagh A, Ibrahim F, Szabados L, et al. The Role of Integrated Positron Emission Tomography/Computed Tomography(PET/CT) and Bone Marrow Examination in Staging Large B-Cell Lymphoma[J]. Clin Med Insights Oncol, 2020, 14: 1179554920953091.
[8] Ujjani CS, Hill EM, Wang H, et al. (18) F-FDG PET-CT and trephine biopsy assessment of bone marrow involvement in lymphoma[J]. Br J Haematol, 2016, 174(3): 410-416. doi: 10.1111/bjh.14071
[9] Berthet L, Cochet A, Kanoun S, et al. In newly diagnosed diffuse large B-cell lymphoma, determination of bone marrow involvement with 18F-FDG PET/CT provides better diagnostic performance and prognostic stratification than does biopsy[J]. J Nucl Med, 2013, 54(8): 1244-1250. doi: 10.2967/jnumed.112.114710
[10] Jitani AK, Dutta S, Mandal PK, et al. Utility of 18F-fluorodeoxyglucose PET-CT scan in detecting bone marrow involvement in lymphoma[J]. Indian J Med Res, 2021, 154(5): 691-698. doi: 10.4103/ijmr.IJMR_1420_19
[11] Vishnu P, Wingerson A, Lee M, et al. Utility of Bone Marrow Biopsy and Aspirate for Staging of Diffuse Large B Cell Lymphoma in the Era of Positron Emission Tomography With 2-Deoxy-2-[Fluorine-18]fluoro-deoxyglucose Integrated With Computed Tomography[J]. Clin Lymphoma Myeloma Leuk, 2017, 17(10): 631-636. doi: 10.1016/j.clml.2017.06.010
[12] Aguado-Vázquez TM, Olivas-Martínez A, Cancino-Ramos U, et al. 18f-Fluorodeoxyglucose Positron Emission Tomography Versus Bone Marrow Biopsy for the Evaluation of Bone Marrow Infiltration in Newly Diagnosed Lymphoma Patients[J]. Rev Invest Clin, 2021, 73(2): 79-86.
[13] Büyükşimşek M, Kolsuz İ, Yetişir AE, et al. Performance of Positron Emission Tomography-Computed Tomography and Bone Marrow Biopsy in Detecting Bone Marrow Infiltration in Lymphoma Cases[J]. Turk J Haematol, 2020, 37(4): 220-225. doi: 10.4274/tjh.galenos.2020.2019.0361
[14] Göçer M, Kurtoǧlu E. Comparison of Bone Marrow Involvement with Bone Marrow Biopsy and PET-CT and Evaluation of Any Effects on Survival in Patients Diagnosed with Hodgkin and Non-Hodgkin Lymphoma[J]. Indian J Hematol Blood Transfus, 2021, 37(1): 52-59. doi: 10.1007/s12288-020-01284-x
[15] Adams HJ, Kwee TC, Fijnheer R, et al. Bone marrow 18F-fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography cannot replace bone marrow biopsy in diffuse large B-cell lymphoma[J]. Am J Hematol, 2014, 89(7): 726-731. doi: 10.1002/ajh.23730
[16] Saiki Y, Tomita N, Uchida A, et al. Biopsy remains indispensable for evaluating bone marrow involvement in DLBCL patients despite the use of positron emission tomography[J]. Int J Hematol, 2021, 113(5): 675-681. doi: 10.1007/s12185-021-03080-3
[17] Wang J, Kim D, Kang WJ, et al. Prognostic Value of Bone Marrow F-18 FDG Uptake in Patients with Advanced-Stage Diffuse Large B-Cell Lymphoma[J]. Nucl Med Mol Imaging, 2020, 54(1): 28-34. doi: 10.1007/s13139-019-00630-w
[18] Chen-Liang TH, Martin-Santos T, Jerez A, et al. The role of bone marrow biopsy and FDG-PET/CT in identifying bone marrow infiltration in the initial diagnosis of high grade non-Hodgkin B-cell lymphoma and Hodgkin lymphoma. Accuracy in a multicenter series of 372 patients[J]. Am J Hematol, 2015, 90(8): 686-690. doi: 10.1002/ajh.24044
[19] Alzahrani M, El-Galaly TC, Hutchings M, et al. The value of routine bone marrow biopsy in patients with diffuse large B-cell lymphoma staged with PET/CT: a Danish-Canadian study[J]. Ann Oncol, 2016, 27(6): 1095-1099. doi: 10.1093/annonc/mdw137
[20] Alonso-Álvarez S, Alcoceba M, García-Álvarez M, et al. Biological Features and Prognostic Impact of Bone Marrow Infiltration in Patients with Diffuse Large B-Cell Lymphoma[J]. Cancers(Basel), 2020, 12(2): 474.
[21] Sehn LH, Scott DW, Chhanabhai M, et al. Impact of concordant and discordant bone marrow involvement on outcome in diffuse large B-cell lymphoma treated with R-CHOP[J]. J Clin Oncol, 2011, 29(11): 1452-1457. doi: 10.1200/JCO.2010.33.3419
[22] Shim H, Oh JI, Park SH, et al. Prognostic impact of concordant and discordant cytomorphology of bone marrow involvement in patients with diffuse, large, B-cell lymphoma treated with R-CHOP[J]. J Clin Pathol, 2013, 66(5): 420-425. doi: 10.1136/jclinpath-2012-201158
[23] Chen Y, Zhou M, Liu J, et al. Prognostic Value of Bone Marrow FDG Uptake Pattern of PET/CT in Newly Diagnosed Diffuse Large B-cell Lymphoma[J]. J Cancer, 2018, 9(7): 1231-1238. doi: 10.7150/jca.23714
[24] Lim CH, Hyun SH, Cho YS, et al. Prognostic significance of bone marrow 2-[18F]-fluoro-2-deoxy-d-glucose uptake in diffuse large B-cell lymphoma: relation to iliac crest biopsy results[J]. Clin Radiol, 2021, 76(7): 550. e19-550.e28. doi: 10.1016/j.crad.2021.02.023
[25] Özpolat HT, Yilmaz E, Goksoy HS, et al. Detection of bone marrow involvement with FDG PET/CT in patients with newly diagnosed lymphoma[J]. Blood Res, 2018, 53(4): 281-287. doi: 10.5045/br.2018.53.4.281
[26] 沈子园, 闫冬梅, 李炳宗, 等. 207例原发性阳性弥漫大B细胞淋巴瘤临床病理特征和预后分析: 一项淮海淋巴瘤工作组多中心回顾性研究[J]. 临床血液学杂志, 2022, 35(9): 656-662. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXZ202209010.htm
-
图(2)
表(2)
计量
- 文章访问数: 1079
- PDF下载数: 414
- 施引文献: 0