
Comparative analysis of perioperative period between splenic embolization and splenectomy for children with hereditary spherocytosis
-
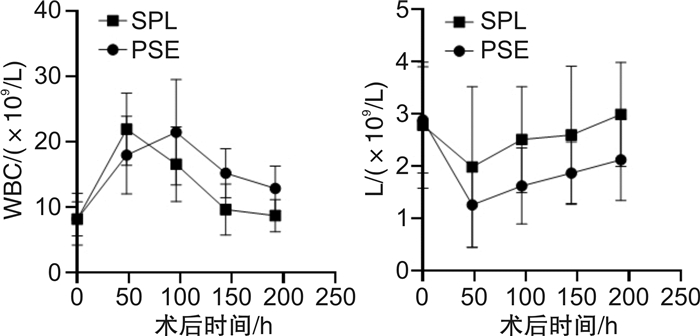
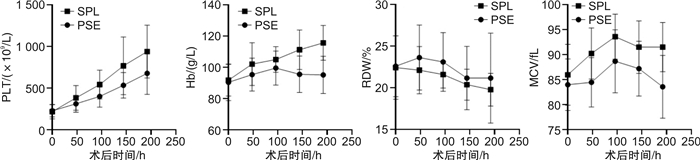
摘要: 目的 比较分析遗传性球形红细胞增多症(hereditary spherocytosis,HS)儿童的血液学参数等指标在脾栓塞术(partial splenic embolization,PSE)与脾切除术(splenectomy,SPL)治疗围手术期的变化趋势及差异。方法 回顾性收集重庆医科大学附属儿童医院2013年8月至2021年8月收治的51例HS儿童围手术期的临床资料,其中26例行PSE,25例行SPL。比较分析2组围手术期血红蛋白(Hb)、红细胞体积分布宽度(RDW)、平均红细胞体积(MCV)、血小板计数(PLT)、住院时间等指标的变化。结果 PSE组术后Hb最高为(95.18±11.93) g/L,与术前Hb比较差异无统计学意义(P>0.05);SPL组术后Hb最高为(115.71±11.12) g/L,与术前比较明显升高(P < 0.05)。且SPL组术后Hb升高较PSE组显著,MCV也升高更明显(P < 0.05)。PSE组RDW由(22.60±3.65)%下降至(21.17±5.40)%;SPL组RDW由术前(22.43±3.80)%降至(19.78±1.97)%(P < 0.05)。2组RDW最低值比较差异有统计学意义(P < 0.05)。PSE组PLT最高为678.13×109/L±252.99×109/L,显著低于SPL组的983.95×109/L±319.93×109/L(P < 0.05),在统计期末无下降趋势。PSE组儿童术后住院时间中位数小于SPL组(P < 0.05)。结论 PSE较SPL更微创、安全,可减少住院天数。PSE组围手术期血液学参数变化趋势更平缓;而RDW的围手术期走势是儿童HS的特异表现。
-
关键词:
- 儿童遗传性球形红细胞增多症 /
- 脾栓塞 /
- 脾切除 /
- 血液学参数 /
- 围手术期
Abstract: Objective To analyze the trends and differences of hematological parameters in the children with hereditary spherocytosis(HS) who treated by splenic embolization or splenectomy during the perioperative period.Methods The perioperative clinical data of 51 children with HS from August 2013 to August 2021 were retrospectively collected. 26 children underwent PSE and 25 children underwent SPL. The changes of hematological and others indexes during the perioperative period of the two groups were analyzed.Results The highest hemoglobin(Hb) values postoperative in PSE group was(95.18±11.93) g/L, there wa no significant difference compared with preoperative values(P>0.05). The highest Hb values postoperative in the SPL group was(115.71±11.12) g/L, and had significant difference(P < 0.05). In addition, the postoperative Hb level increased in SPL group was significantly higher than that in PSE group, and the MCV level was also significantly higher(P < 0.05). RDW decreased from(22.60±3.65)% to (21.17±5.40)% in PSE group, and decreased from(22.43±3.80)% to (19.78±1.97)% in SPL group(P < 0.05). The highest PLT values of PSE group was 678.13×109/L±252.99×109/L, which was significantly lower than that in SPL group 983.95×109/L±319.93×109/L(P < 0.05), and there was no decreasing trend at the end of the statistical period. The median postoperative hospital length of stays in PSE group was less than that in SPL group(P < 0.05).Conclusion PSE may be more minimally invasive and safer than SPL, and can reduce the length of hospital stay. It's a characteristic of HS in children what the perioperative trend of RDW. -

-
表 1 2组患儿各项指标比较
指标 中位数 P 年龄/岁 PSE 7.0(5.0~8.0) SPL 9.0(7.0~11.5) 住院时间/d < 0.05 PSE 9(7~13) SPL 13(10~17) Hb/(g/L) 术前PSE 88.00(84.50~94.00) 术前SPL 93.70(85.50~98.50) WBC/(×109/L) 术前PSE 7.95(6.11~10.83) 术前SPL 7.20(5.15~10.46) 术后PSE峰值 23.93(16.72~26.29) 术后SPL峰值 23.61(14.35~26.09) 达峰时间/d < 0.05 PSE 3(2~3) SPL 1(1~2) PLT/(×109/L) < 0.05 术前PSE 220.50(181.75~273.75) 术前SPL 225.00(160.50~270.50) 术后PSE峰值 726.50(570.75~1 037.50) 术后SPL峰值 1 020.00(684.50~1 399.00) PLT > 1 000/例(%) < 0.05 PSE 2(7.6) SPL 9(36.0) 胆红素/(μmol/L) < 0.05 术前PSE 67.35(41.15~96.80) 术前SPL 56.80(48.68~76.00) 术后48 h PSE 39.55(19.95~52.50) 术后48 h SPL 19.10(12.43~24.12) 发热/例(%) < 0.05 PSE 12(46) SPL 13(52) 术后开始发热时间/d PSE 3(2~3) SPL 1(1~2) 发热持续时间/d < 0.05 PSE 3.5(3.0~4.0) SPL 1.0(1.0~2.0)  下载: 导出CSV
下载: 导出CSV
-
[1] Perrotta S, Gallagher PG, Mohandas N. Hereditary spherocytosis[J]. Lancet, 2008, 372(9647): 1411-1426. doi: 10.1016/S0140-6736(08)61588-3
[2] Iolascon A, Andolfo I, Barcellini W, et al. Recommendations regarding splenectomy in hereditary hemolytic anemias[J]. Haematologica, 2017, 102(8): 1304-1313. doi: 10.3324/haematol.2016.161166
[3] Luu S, Spelman D, Woolley IJ. Post-splenectomy sepsis: preventative strategies, challenges, and solutions[J]. Infect Drug Resist, 2019, 12: 2839-2851. doi: 10.2147/IDR.S179902
[4] Crary SE, Buchanan GR. Vascular complications after splenectomy for hematologic disorders[J]. Blood, 2009, 114(14): 2861-2868. doi: 10.1182/blood-2009-04-210112
[5] Kimura F, Ito H, Shimizu H, et al. Partial splenic embolization for the treatment of hereditary spherocytosis[J]. Am J Roentgenol, 2003, 181: 1021-1024. doi: 10.2214/ajr.181.4.1811021
[6] Pratl B, Benesch M, Lackner H, et al. Partial splenic embolization in children with hereditary spherocytosis[J]. Eur J Haematol, 2007, 80(1): 76-80. http://onlinelibrary.wiley.com/doi/10.1111/j.1600-0609.2007.00979.x/pdf
[7] Wang RJ, Xiao L, Xu XM, et al. Super-Selective Partial Splenic Embolization for Hereditary Spherocytosis in Children: A Single-Center Retrospective Study[J]. Front Surg, 2022, 9: 835430. doi: 10.3389/fsurg.2022.835430
[8] Bolton-Maggs PH, Langer JC, Iolascon A, et al. Guidelines for the diagnosis and management of hereditary spherocytosis-2011 update[J]. Br J Haematol, 2012, 156(1): 37-49. doi: 10.1111/j.1365-2141.2011.08921.x
[9] Gallagher PG. Abnormalities of the erythrocyte membrane[J]. Pediatr Clin North Am, 2013, 60(6): 1349-1362. doi: 10.1016/j.pcl.2013.09.001
[10] 潘美秀, 韦松晓, 林伟健, 等. 血液学指标在4种常见α地中海贫血中筛查价值[J]. 临床血液学杂志, 2022, 35(4): 283-286. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXZ202204012.htm
[11] Wernick B, Cipriano A, Odom SR, et al. Temporal changes in hematologic markers after splenectomy, splenic embolization, and observation for trauma[J]. Eur J Trauma Emerg Surg, 2017, 43(3): 399-409. doi: 10.1007/s00068-016-0679-0
[12] Skattum J, Titze TL, Dormagen JB, et al. Preserved splenic function after angioembolisation of high grade injury[J]. Injury, 2012, 43(1): 62-66. doi: 10.1016/j.injury.2010.06.028
[13] Theodorou GL, Mouzaki A, Tsiftsis D, et al. Effect of non-operative management(NOM)of splenic rupture versus splenectomy on the distribution of peripheral blood lymphocyte populations and cytokine production by T cells[J]. Clin Exp Immunol, 2007, 150(3): 429-436. doi: 10.1111/j.1365-2249.2007.03517.x
-
图(3)
表(1)
计量
- 文章访问数: 788
- PDF下载数: 238
- 施引文献: 0