
Exploring the prevention status of venous thromboembolism in Chinese multiple myeloma based on single-center real-world data and the predictive value of related risk stratification systems
-
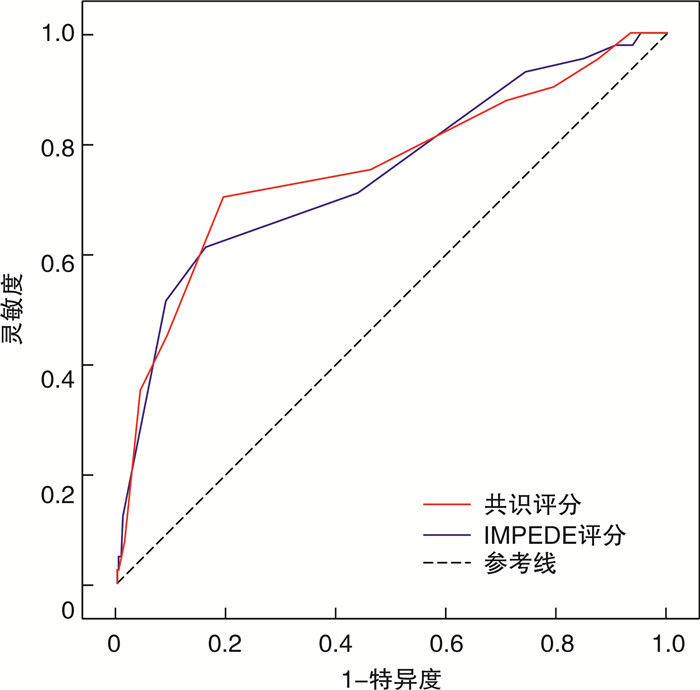
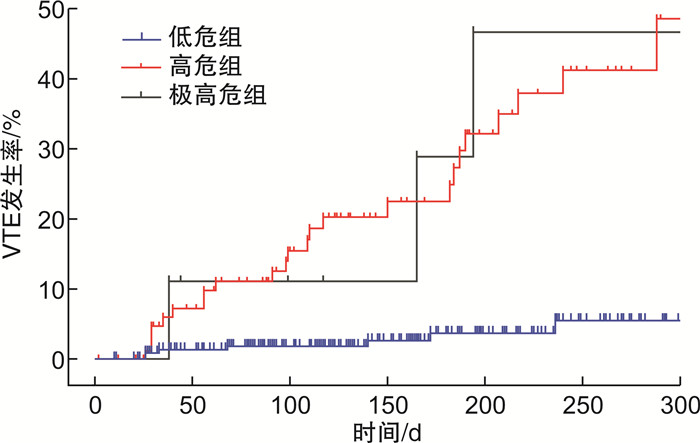
摘要: 目的 通过统计真实世界中多发性骨髓瘤(multiple myeloma,MM)患者静脉血栓栓塞症(venous thromboembolism,VTE)的预防措施和发生情况,探讨目前中国MM相关VTE预防存在的问题,并初步检验《多发性骨髓瘤相关静脉血栓栓塞症防治中国专家共识(2022年版)》提出的VTE风险评分系统(简称为中国共识风险评分系统)对中国新诊断多发性骨髓瘤患者(newly diagnosed multiple myeloma,NDMM)发生VTE的预测效能。方法 收集并分析2018年1月—2023年8月在医院诊断的NDMM患者的临床资料,包括患者基本特征、VTE预防用药以及是否出现VTE,根据中国共识风险评分系统对患者进行风险评估,并统计VTE事件发生率,根据受试者工作特征曲线的曲线下面积与IMPEDE模型的预测效能进行对比。结果 共428例NDMM患者,VTE发生率为9.58%,低危组、高危组和极高危组的VTE发生率分别为3.35%、26.60%和40.00%,低危组与高危组和极高危组之间的VTE发生率差异有统计学意义(P<0.05);低危组中170例患者给予了血栓预防,164例使用阿司匹林,6例使用抗凝剂,高危组中60例患者给予了血栓预防,其中57例使用阿司匹林,3例使用抗凝剂,低危组与高危组患者使用阿司匹林比例分别为68.62%和60.64%。中国共识风险评分系统和IMPEDE模型预测NDMM患者VTE的受试者工作特征曲线(ROC)下面积(AUC)分别为0.760(0.670~0.850)和0.685(0.591~0.780),敏感度分别为70.70%和73.20%,特异度分别为80.60%和59.40%。结论 中国共识风险评分系统可以明显区分低危、高危及极高危患者,且预测效能优于IMPEDE模型,中国血液科医师对于MM相关VTE的分层预防的认识有待进一步提高,合理地预防用药需要更多的临床数据进行探索。Abstract: Objective To investigate the prevention measures and occurrence of venous thromboembolism(VTE) in patients with multiple myeloma(MM) based on real-world data. It examines the existing issues in VTE prevention in Chinese MM patients and preliminarily tests the predictive efficacy of the VTE risk score system proposed in the Consensus on the Prevention and Treatment of Venous Thromboembolism in Multiple Myeloma in China(2022 Edition), referred to as the Chinese Consensus Risk Score System, for the occurrence of VTE in newly diagnosed multiple myeloma(NDMM) patients in China.Methods Clinical data of NDMM patients diagnosed at our hospital between January 2018 and August 2023 was collected and analyzed, including patients' baseline characteristics, VTE prophylactic medications, and the occurrence of VTE. Patients were assessed for risk using the Chinese Consensus Risk Score System, and the incidence of VTE will be calculated. The predictive effectiveness of the system was compared with the IMPEDE model using the area under the receiver operating characteristic curve.Results Among 428 NDMM patients, the incidence of VTE was 9.58%. The VTE incidence in the low-risk, high-risk, and very high-risk groups was 3.35%, 26.60%, and 40.00%, respectively. There was a statistically significant difference in VTE incidence between the low-risk group and the high-risk/very high-risk group(P < 0.05). In the low-risk group, 170 patients received thromboprophylaxis, with 164 using aspirin and 6 using anticoagulants. In the high-risk group, 60 patients received thromboprophylaxis, with 57 using aspirin and 3 using anticoagulants. The proportion of patients using aspirin was 68.62% and 60.64% in the low-risk and high-risk groups, respectively. The Chinese Consensus Risk Score System and the IMPEDE model had receiver operating characteristic (ROC) curve areas under the curve (AUC) of 0.760 (0.670-0.850) and 0.685 (0.591-0.780), respectively. The sensitivity was 70.70% and 73.20%, and the specificity was 80.60% and 59.40%, respectively.Conclusion The Chinese Consensus Risk Score System can effectively differentiate low-risk, high-risk, and very high-risk patients, and it has better predictive efficacy than the IMPEDE model. The understanding of stratified prevention of MM-related VTE among Chinese hematologists needs further improvement, and rational prevention medication requires more exploration with clinical data.
-
Key words:
- multiple myeloma /
- venous thromboembolism /
- risk assessment /
- thromboprophylaxis
-

-
表 1 中国共识风险评分量表[14]
危险因素 积分 个体和疾病因素 遗传性易栓症 6 VTE家族史 5 VTE病史 5 狼疮抗凝物阳性 4 骨盆、臀部或股骨骨折 4 浅静脉血栓病史 3 患者需要卧床超过72 h 2 大手术(1个月内) 2 抗心磷脂抗体阳性 2 年龄>75岁 2 年龄60~75岁 1 体质指数≥25 kg/m[2] 1 M蛋白浓度≥30 g/L 1 充血性心力衰竭(1个月内) 1 急性心肌梗死 1 肺功能异常(慢性阻塞性肺疾病) 1 糖尿病 1 肾病综合征 1 治疗因素 免疫调节 4 每周期地塞米松总量>160 mg 4 每周期地塞米松总量120~160 mg 2 蒽环类为主的多药化疗 3 卡非佐米 2 中心静脉置管 2 促红细胞生成素 1  下载: 导出CSV
下载: 导出CSV
表 2 IMPEDE风险评分量表[19]
危险因素 积分 正在使用免疫调节剂类药物 4 体质指数≥25 kg/m[2] 1 骨盆、髋部或股骨骨折 4 使用促红细胞生成剂治疗 1 使用多柔比星治疗 3 地塞米松治疗剂量 大剂量地塞米松 4 小剂量地塞米松 2 种族/人种=亚洲/太平洋岛民 -3 在多发性骨髓瘤发生前有VTE史 5 有隧道式导管/中央静脉置管 2 正在进行血栓预防措施:治疗应用低分子量肝素或华法林 -4 正在进行血栓预防措施:如治疗应用低分子量肝素或阿司匹林 -3
下载: 导出CSV
表 3 428例患者一般情况
类型 例(%) 性别 男 253(59.11) 女 175(40.89) 年龄/岁 58.68±9.42 <60 233(54.44) ≥60 195(45.56) ECOG评分/分 0~2 385(89.95) >2 43(10.05) BMI/(kg/m[2]) <25 390(91.12) ≥25 38(8.88) 既往史 VTE 9(2.10) COPD 13(3.04) 高血压病 80(18.69) 冠心病 14(3.27) 脑血管疾病 12(2.80) 慢性肾脏病 12(2.80) 糖尿病 27(6.31) 手术外伤史 107(25.00) 抗血栓药物史 34(7.94) 卧床≥72 h 5(1.17) M蛋白/(g/L) 32.12±27.68 轻链型 78(18.22) 不分泌 6(1.40) β2-微球蛋白/(mg/L) 10.57±15.50 FISH异常 t(4;14) 72(16.82) t(14;16) 26(6.07) t(14;20) 54(12.62) del(17p) 44(10.28) ISS分期 Ⅰ期 122(28.50) Ⅱ期 99(23.13) Ⅲ期 187(43.69) R-ISS分期 Ⅰ期 69(16.12) Ⅱ期 219(51.17) Ⅲ期 97(22.66) 免疫调节剂 来那度胺 216(50.47) 沙利度胺 47(10.98) 泊马度胺 36(8.41) 卡非佐米 20(4.67) 促红细胞生成素 240(56.07) 中心静脉置管 252(58.88)
下载: 导出CSV
表 4 依据中国共识风险评分系统分层后NDMM患者的血栓预防情况和VTE事件
例 组别 低危组 高危组 极高危组 总例数 VTE 总例数 VTE 总例数 VTE 未预防 69 4 34 12 3 1 阿司匹林 164 4 57 12 3 2 抗凝剂 6 0 3 1 4 0
下载: 导出CSV
-
[1] Palumbo A, Rajkumar SV, Dimopoulos MA, et al. Prevention of thalidomide-and lenalidomide-associated thrombosis in myeloma[J]. Leukemia, 2008, 22(2): 414-423. doi: 10.1038/sj.leu.2405062
[2] Harousseau JL, Dreyling M, ESMO Guidelines Working Group. Multiple myeloma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up[J]. Ann Oncol, 2010, 2021, 32(3): 309-322.
[3] Fotiou D, Gavriatopoulou M, Terpos E. Multiple myeloma and thrombosis: prophylaxis and risk prediction tools[J]. Cancers, 2020, 12(1): 191. doi: 10.3390/cancers12010191
[4] Larocca A, Cavallo F, Bringhen S, et al. Aspirin or enoxaparin thromboprophylaxis for patients with newly diagnosed multiple myeloma treated with lenalidomide[J]. Blood, 2012, 119(4): 933-939;quiz 1093. doi: 10.1182/blood-2011-03-344333
[5] 赵冰妮, 杨林花. 多发性骨髓瘤合并静脉血栓栓塞症的研究进展[J]. 临床血液学杂志, 2022, 35(5): 383-387, 392. https://lcxy.whuhzzs.com/article/doi/10.13201/j.issn.1004-2806.2022.05.017
[6] Li PP, Xu B, Xu JD, et al. Thrombosis events in Chinese patients with newly diagnosed multiple myeloma[J]. Clin Exp Med, 2023, 23(7): 3809-3820. doi: 10.1007/s10238-023-01080-7
[7] Raghupathy R, Ayyappan S, Prabhakar D, et al. Retrospective study of the incidence and patterns of arterial and venous thrombosis in Chinese versus African American patients with multiple myeloma[J]. Br J Haematol, 2017, 176(2): 315-317. doi: 10.1111/bjh.13942
[8] Cowan AJ, Green DJ, Kwok M, et al. Diagnosis and management of multiple myeloma: a review[J]. JAMA, 2022, 327(5): 464-477. doi: 10.1001/jama.2022.0003
[9] Silberstein J, Tuchman S, Grant SJ. What Is Multiple Myeloma?[J]. JAMA, 2022, 327(5): 497. doi: 10.1001/jama.2021.25306
[10] Rajkumar SV. Multiple myeloma: Every year a new standard?[J]. Hematol Oncol, 2019, 37(Suppl 1): 62-65.
[11] Li XZ, Sun XL, Fang BJ, et al. Development and validation of a new risk assessment model for immunomodulatory drug-associated venous thrombosis among Chinese patients with multiple myeloma[J]. Thromb J, 2023, 21(1): 105. doi: 10.1186/s12959-023-00534-y
[12] Guzdar A, Costello C. Supportive care in multiple myeloma[J]. Curr Hematol Malig Rep, 2020, 15(2): 56-61. doi: 10.1007/s11899-020-00570-9
[13] Li Q, Zhang B, Cheng QW, et al. Hematologists' awareness of venous thromboembolism in multiple myeloma: a national survey in China[J]. Ann Med, 2023, 55(2): 2263019. doi: 10.1080/07853890.2023.2263019
[14] 中华医学会血液学分会浆细胞疾病学组, 中华医学会血液学分会血栓与止血学组. 多发性骨髓瘤相关静脉血栓栓塞症防治中国专家共识(2022年版)[J]. 中华血液学杂志, 2022, 43(9): 726-731. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXZ202307001.htm
[15] 唐亮, 胡豫. 《多发性骨髓瘤相关静脉血栓栓塞症防治中国专家共识(2022年版)》解读[J]. 临床血液学杂志, 2023, 36(7): 457-460. https://lcxy.whuhzzs.com/article/doi/10.13201/j.issn.1004-2806.2023.07.001
[16] Ho M, Patel A, Goh CY, et al. Changing paradigms in diagnosis and treatment of monoclonal gammopathy of undetermined significance(MGUS)and smoldering multiple myeloma(SMM)[J]. Leukemia, 2020, 34(12): 3111-3125. doi: 10.1038/s41375-020-01051-x
[17] 中国医师协会血液科医师分会, 中华医学会血液学分会. 中国多发性骨髓瘤诊治指南(2022年修订)[J]. 中华内科杂志, 2022, 61(5): 480-487. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXZ201611020.htm
[18] 马军, 秦叔逵, 吴一龙, 等. 肿瘤相关静脉血栓栓塞症预防与治疗指南(2019版)[J]. 中国肿瘤临床, 2019, 46(13): 653-660. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGZL201913001.htm
[19] Fotiou D, Dimopoulos MA, Kastritis E. Approach to contemporary risk assessment, prevention and management of thrombotic complications in multiple myeloma[J]. Cancers(Basel), 2022, 14(24): 6216.
[20] Bradbury CA, Craig Z, Cook G, et al. Thrombosis in patients with myeloma treated in the Myeloma Ⅸ and Myeloma Ⅺ phase 3 randomized controlled trials[J]. Blood, 2020, 136(9): 1091-1104. http://www.sciencedirect.com/science/article/pii/S0006497120617645
[21] 王春晖, 魏征, 李晓宇, 等. 一项多发性骨髓瘤患者应用免疫调节药物致静脉血栓事件危险因素和预防情况的回顾性研究[J]. 肿瘤药学, 2023, 13(3): 353-360. https://www.cnki.com.cn/Article/CJFDTOTAL-LIYX202303014.htm
[22] 房立娟, 姚晓东, 陆敏秋, 等. Padua与IMPEDE评估量表在新诊断多发性骨髓瘤患者静脉血栓栓塞症预测中的比较研究: 单中心数据[J]. 中华血液学杂志, 2023, 44(5): 395-400. https://www.cnki.com.cn/Article/CJFDTOTAL-YYPF202403004.htm
[23] Swan D, Comerford C, Quinn J. Venous thromboembolism in multiple myeloma: Increasing evidence in support of direct oral anticoagulants[J]. Br J Haematol, 2023, 203(3): 351-352.
-
图(2)
表(4)
计量
- 文章访问数: 1354
- PDF下载数: 437
- 施引文献: 0