
-
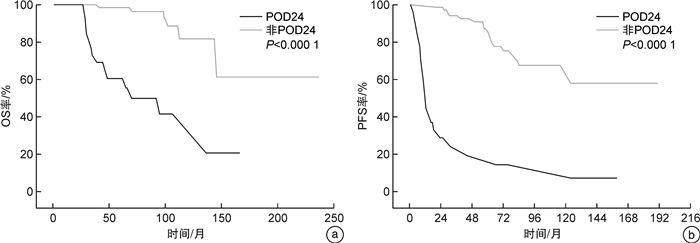
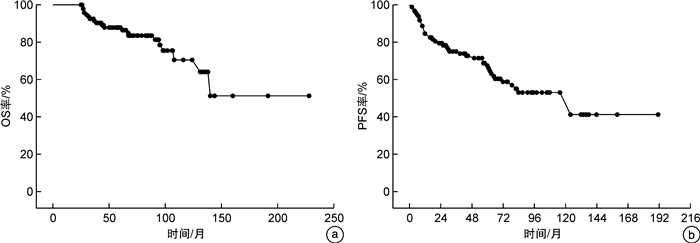
摘要: 目的 探讨24个月内疾病进展(POD24)对霍奇金淋巴瘤(Hodgkin lymphoma,HL)患者总生存期(overall survival,OS)的影响,比较POD24组和非POD24组的临床特征以及分析影响POD24的相关危险因素。方法 回顾性分析2004年1月—2021年8月徐州医科大学附属医院确诊为HL且经过正规治疗的98例患者,进行预后评估及临床特征分析。结果 共纳入患者98例。所有患者的中位OS和PFS分别为75.3(25.0~228.0)个月和60.0(2.0~192.0)个月。其中POD24组27例,该组的中位OS和中位PFS分别为52.0(25.0~160.0)个月和12.0(2.0~160.0)个月,非POD24组的中位OS和PFS分别为84.0(25.0~228.0)个月和70.0(20.0~192.0)个月。单因素分析显示POD24、白蛋白(< 40 g/L)、血红蛋白(< 100 g/L)、血清β2-微球蛋白(>2.366 mg/L)、IPI评分0~2分、初次化疗后的治疗反应、年龄>60岁以及美国东部肿瘤协作组(ECGO)体能状态(PS)评分0~1分为与总生存相关的不良预后因素。多因素分析提示POD24(P < 0.001)、白蛋白(< 40 g/L) (P=0.011)、年龄>60岁(P=0.022)以及初始治疗后疾病达缓解(P=0.005)有独立预后意义。本组资料显示,非POD24组初次化疗后病情缓解的患者为63例,POD24组13例,此外,POD24组与非POD24组Ann Arbor分期、IPI评分、β2-微球蛋白、ECOG PS评分等特征差异有统计学意义(P<0.05)。结论 POD24为HL患者OS的独立预后不良因素,Ann Arbor分期Ⅲ/Ⅳ期以及初次化疗后的病情未缓解的患者发生POD24比例更高,而IPI评分0~2分、ECOG评分0~1分的患者发生POD24的比例更低。Abstract: Objective To explore the effect of progression of disease within 24 months(POD24) on overall survival(OS) of Hodgkin lymphoma(HL), compare to the clinical characteristics between POD24 HL with non-POD24 HL patients, and analyze the related risk factors affecting POD24.Methods The patients with HL who were treated in the Affiliated Hospital of Xuzhou Medical University from January 2004 to August 2021 were retrospectively analyzed, and their prognosis and clinical characteristics were evaluated.Results A total of 98 patients with HL were included. The median OS and PFS of all patients were 75.3(25.0-228.0) months and 60.0(2.0-192.0) months, respectively. Among them, there were 27 patients in the POD24 group. The median OS and PFS of thePOD24 group were 52.0(25.0-160.0) months and 12.0(2.0-160.0) months, The median OS and PFS of the non-POD24 group were 84.0(25.0-228.0) months and 70.0(20.0-192.0) months respectively. Univariate analysis showed that POD24, albumin(< 40 g/L), hemoglobin(< 100 g/L), serum β2 microglobulin(>2.366 mg/L), IPI score 0-2, treatment response after initial chemotherapy, age>60 years, and Eastern Cooperative Oncology Group(ECGO) physical status(PS) score 0-1 were adverse prognostic factors associated with overall survival(OS). Multivariate analysis showed that POD24(P < 0.001), albumin(< 40 g/L)(P=0.011), age>60 years(P=0.022) and remission after initial treatment(P=0.005) had independent prognostic significance. According to the data of this group, 63 patients in the non-POD24 group had remission after initial chemotherapy, while only 13 patients in the POD24 group. In addition, there were significant differences in Ann Arbor staging, IPI score, serum β2 microglobulin, and ECOG PS score between the POD24 group and the non-POD24 group(P < 0.05).Conclusion POD24 is an independent poor prognostic factor for the OS of HL patients. The proportion of patients with Ann Arbor stage Ⅲ/Ⅳ and unresponsive disease after initial chemotherapy was higher in the POD24 group, while patients with IPI score 0-2 and ECGO score 0-1 have a lower proportion of POD24.
-
Key words:
- Hodgkin lymphoma /
- early disease progression /
- POD24 /
- overall survival /
- prognostic analysis
-

-
表 1 98例患者的基本临床特征
特征 总例数(n=98) POD24组(n=27) 非POD24组(n=71) P 年龄/岁 34.7(17.0~79.0) 44.0(18.0~76.0) 31.6(17.0~79.0) 年龄/例(%) 0.906 >60岁 21(21.4) 6(22.2) 15(21.1) ≤60岁 77(78.6) 21(77.8) 56(78.9) 性别/例(%) 0.690 男 54(55.1) 14(51.9) 40(56.3) 女 44(44.9) 13(48.1) 31(43.7) Ann Arbor分期/例(%) 0.008 Ⅰ/Ⅱ 35(35.7) 4(14.8) 31(43.7) Ⅲ/Ⅳ 63(64.3) 23(85.2) 40(56.3) ECOG评分/例(%) 0.048 0~1 89(90.8) 22(81.5) 67(94.4) 2~4 9(9.2) 5(18.5) 4(5.6) B症状/例(%) 0.215 是 41(41.8) 14(51.9) 27(38.0) 否 57(58.2) 13(48.1) 44(62.0) IPI评分/例(%) 0.008 0~2 73(74.5) 15(55.6) 58(81.7) 3~5 25(25.5) 12(44.4) 13(18.3) 血红蛋白水平/例(%) 0.107 ≥100 g/L 85(86.7) 21(77.8) 64(90.1) < 100 g/L 13(13.3) 6(22.2) 7(9.9) 血小板计数/例(%) 0.522 ≥125×109/L 93(94.9) 25(92.6) 68(95.8) < 125×109/L 5(5.1) 2(7.4) 3(4.2) 白细胞计数/例(%) 0.522 ≥3.5×109/L 93(94.9) 25(92.6) 68(95.8) < 3.5×109/L 5(5.1) 2(7.4) 3(4.2) 淋巴细胞计数/例(%) 0.329 ≥1.0×109/L 62(63.3) 15(55.6) 47(66.2) < 1.0×109/L 36(36.7) 12(44.4) 24(33.8) β2-微球蛋白/例(%) 0.030 < 2.366 mg/L 67(68.4) 14(51.9) 53(74.6) ≥2.366 mg/L 31(31.6) 13(48.1) 18(25.4) 血沉/例(%) 0.857 < 15 mm/h 23(23.5) 6(22.2) 17(23.9) ≥15 mm/h 75(76.5) 21(77.8) 54(76.1) 白蛋白水平/例(%) 0.709 ≥40 g/L 53(54.1) 13(48.1) 32(45.1) < 40 g/L 45(45.9) 14(51.9) 39(54.9) LDH水平/例(%) 0.823 < 240 U/L 67(68.4) 18(66.7) 49(69.0) ≥240 U/L 31(31.6) 9(33.3) 22(31.0) 骨髓侵犯/例(%) 0.723 是 23(23.5) 7(25.9) 16(22.5) 否 75(76.5) 20(74.1) 55(77.5) 淋巴结外侵犯部位>2/例(%) 0.580 是 14(14.3) 3(11.1) 11(15.5) 否 84(85.7) 24(88.9) 60(84.5) CRP水平/例(%) 0.709 ≥5 mg/L 67(68.4) 19(70.4) 48(67.6) < 5 mg/L 31(31.6) 8(29.6) 23(32.4) 初次化疗后疗效/例(%) < 0.001 CR+PR 76(77.6) 13(48.1) 63(88.7) PD+SD 22(19.4) 14(51.9) 8(11.3) 组织学亚型/例(%) 0.264 混合细胞型 39(39.8) 11(40.7) 28(39.4) 结节硬化型 45(45.9) 10(37.0) 35(49.3) 淋巴细胞丰富型 13(13.3) 5(18.5) 8(11.3) 淋巴细胞消减型 1(1.0) 1(3.7) 0 治疗方案/例(%) 0.329 单纯化疗 62(63.3) 15(55.6) 47(66.2) 联合治疗 36(36.7) 12(44.4) 24(33.8)  下载: 导出CSV
下载: 导出CSV
表 2 影响患者OS的单因素和多因素分析
类型 单因素 多因素 HR(95%CI) P HR(95%CI) P 年龄>60岁 2.686(1.063~6.787) 0.037 5.864(1.284~26.773) 0.022 男/女 1.104(0.499~2.713) 0.829 Ann Arbor分期Ⅲ/Ⅳ期 3.037(0.988~9.338) 0.053 存在B症状 0.858(0.341~2.161) 0.746 ECOG评分0~1分 0.182(0.064~0.514) 0.001 0.514(0.122~2.167) 0.365 IPI评分0~2分 0.128(0.048~0.340) < 0.001 0.662(0.168~2.607) 0.556 β2-微球蛋白≥2.366 mg/L 3.227(1.333~7.814) 0.009 0.920(0.205~4.120) 0.913 白蛋白 < 40 g/L 3.747(1.347~10.423) 0.011 4.928(1.436~16.912) 0.011 LDH≥240 U/L 1.303(0.529~3.208) 0.564 CRP≥5 mg/L 2.651(0.772~9.099) 0.121 血沉≥15 mm/h 0.688(0.262~1.805) 0.447 血红蛋白 < 100 g/L 4.061(1.539~10.716) 0.005 0.739(0.217~2.513) 0.628 血小板计数 < 125×109/L 3.572(1.032~12.371) 0.045 1.205(0.179~8.092) 0.848 白细胞计数 < 3.5×109/L 1.446(0.190~11.019) 0.722 淋巴细胞计数 < 1.0×109/L 1.762(0.733~4.235) 0.206 骨髓侵犯 1.079(0.351~3.310) 0.895 结外累及 1.390(0.537~3.597) 0.497 混合细胞型 0.755(0.300~1.899) 0.550 结节硬化型 0.719(0.293~1.763) 0.471 疾病缓解 0.115(0.044~0.303) < 0.001 0.150(0.040~0.563) 0.005 POD24 9.672(3.671~25.480) < 0.001 10.969(3.343~35.987) < 0.001
下载: 导出CSV
表 3 影响患者PFS的单因素和多因素分析
类型 单因素 多因素 HR(95%CI) P HR(95%CI) P 年龄>60岁 1.724(0.853~3.483) 0.129 男性/女性 0.900(0.487~1.664) 0.737 Ann Arbor分期Ⅲ/Ⅳ期 2.186(1.070~4.468) 0.032 0.584(0.214~1.591) 0.292 存在B症状 1.199(0.647~2.223) 0.565 ECOG评分0~1分 0.263(0.115~0.604) 0.002 1.513(0.428~5.353) 0.521 IPI评分0~2分 0.263(0.137~0.506) < 0.001 1.279(0.442~3.699) 0.650 β2-微球蛋白≥2.366 mg/L 2.587(1.392~4.810) 0.003 2.548(1.077~6.028) 0.033 白蛋白 < 40 g/L 1.626(0.877~3.013) 0.123 LDH≥240 U/L 1.503(0.801~2.818) 0.564 CRP≥5 mg/L 2.093(0.965~4.538) 0.061 血沉≥15 mm/h 1.057(0.504~2.219) 0.883 血红蛋白 < 100 g/L 2.154(0.991~4.682) 0.053 血小板计数 < 125×109/L 2.670(0.946~7.535) 0.064 白细胞计数 < 3.5×109/L 1.182(0.284~4.911) 0.818 淋巴细胞计数 < 1.0×109/L 1.259(0.676~2.346) 0.468 骨髓侵犯 2.370(1.226~4.584) 0.010 2.226(0.769~6.444) 0.140 结外累及 2.180(1.154~4.121) 0.016 1.152(0.446~2.975) 0.770 混合细胞型 1.215(0.655~2.252) 0.537 结节硬化型 0.763(0.409~1.421) 0.394 POD24 8.736(4.597~16.598) < 0.001 11.278(4.886~26.033) < 0.001 疾病缓解 0.084(0.040~0.176) < 0.001 0.070(0.026~0.192) < 0.001
下载: 导出CSV
-
[1] Ansell SM. Hodgkin lymphoma: 2023 update on diagnosis, risk-stratification, and management[J]. Am J Hematol, 2022, 97(11): 1478-1488. doi: 10.1002/ajh.26717
[2] Vassilakopoulos TP, Asimakopoulos JV, Konstantopoulos K, et al. Optimizing outcomes in relapsed/refractory Hodgkin lymphoma: a review of current and forthcoming therapeutic strategies[J]. Ther Adv Hematol, 2020, 11: 2040620720902911.
[3] Casulo C, Byrtek M, Dawson KL, et al. Early Relapse of Follicular Lymphoma After Rituximab Plus Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone Defines Patients at High Risk for Death: An Analysis From the National LymphoCare Study[J]. J Clin Oncol, 2015, 33(23): 2516-2522. doi: 10.1200/JCO.2014.59.7534
[4] 石远凯. 淋巴瘤[M]. 北京: 北京大学医学出版社, 2007: 34.
[5] 徐卫, 范磊, 缪祎, 等. 江苏省多中心5147例淋巴瘤亚型分析[J]. 中华血液学杂志, 2014, 35(4): 300-303.
[6] 李小秋, 李甘地, 高子芬, 等. 中国淋巴瘤亚型分布: 国内多中心性病例10 002例分析[J]. 诊断学理论与实践, 2012, 11(2): 111-115. https://www.cnki.com.cn/Article/CJFDTOTAL-ZDLS201202007.htm
[7] Wei C, Li W, Qin L, et al. Clinicopathologic characteristics, outcomes, and prognostic factors of angioimmunoblastic T-cell lymphoma in China[J]. Cancer Med, 2023, 12(4): 3987-3998. doi: 10.1002/cam4.5248
[8] 中国抗癌协会血液肿瘤专业委员会, 中华医学会血液学分会, 中国霍奇金淋巴瘤工作组. 中国霍奇金淋巴瘤的诊断与治疗指南(2022年版)[J]. 中华血液学杂志, 2022, 43(9): 705-715.
[9] Punnett A, Tsang RW, Hodgson DC. Hodgkin lymphoma across the age spectrum: epidemiology, therapy, and late effects[J]. Semin Radiat Oncol, 2010, 20(1): 30-44. doi: 10.1016/j.semradonc.2009.09.006
[10] Wang HW, Balakrishna JP, Pittaluga S, et al. Diagnosis of Hodgkin lymphoma in the modern era[J]. Br J Haematol, 2019, 184(1): 45-59. doi: 10.1111/bjh.15614
[11] Liu W, Liu J, Song Y, et al. Burden of lymphoma in China, 2006-2016: an analysis of the Global Burden of Disease Study 2016[J]. J Hematol Oncol, 2019, 12: 115. doi: 10.1186/s13045-019-0785-7
[12] Kuzich JA, Hutchison AP, Lim KJC, et al. Prognostic factors and the impact of frontline therapy in peripheral T-cell lymphoma: 10 years of 'real-world' experience from Western Australia[J]. Leuk Lymphoma, 2019, 60(14): 3417-3425. doi: 10.1080/10428194.2019.1637865
[13] Mottok A. Tumormikromilieu im klassischen Hodgkin-Lymphom[Microenvironment in classical Hodgkin lymphoma][J]. Pathologe, 2020, 41(3): 254-260. doi: 10.1007/s00292-020-00774-z
[14] Ohshima R, Motomura S, Hashimoto C, et al. ABVD chemotherapy for Hodgkin lymphoma at a single institute[J]. Rinsho Ketsueki, 2010, 51(12): 1756-1761.
[15] Bonadonna G, Viviani S, Bonfante V, et al. Survival in Hodgkin's disease patients--report of 25 years of experience at the Milan Cancer Institute[J]. Eur J Cancer, 2005, 41(7): 998-1006. doi: 10.1016/j.ejca.2005.01.006
[16] Liu W, Qi J, Liu J, et al. Mortality Rate of Lymphoma in China, 2013-2020[J]. Front Oncol, 2022, 12: 902643. doi: 10.3389/fonc.2022.902643
[17] Luminari S, Merli M, Rattotti S, et al. Early progression as a predictor of survival in marginal zone lymphomas: an analysis from the FIL-NF10 study[J]. Blood, 2019, 134(10): 798-801. doi: 10.1182/blood.2019001088
[18] 吕瑞, 阎禹廷, 易树华, 等. POD24在106例伴骨髓侵犯脾边缘区淋巴瘤中的预后意义[J]. 中华血液学杂志, 2020, 41(3): 228-233.
[19] Advani RH, Skrypets T, Civallero M, et al. Outcomes and prognostic factors in angioimmunoblastic T-cell lymphoma: final report from the international T-cell Project[J]. Blood, 2021, 138(3): 213-220. doi: 10.1182/blood.2020010387
[20] Weniger MA, Küppers R. Molecular biology of Hodgkin lymphoma[J]. Leukemia, 2021, 35(4): 968-981. doi: 10.1038/s41375-021-01204-6
[21] Flerlage JE, Myers JR, Maciaszek JL, et al. Discovery of novel predisposing coding and noncoding variants in familial Hodgkin lymphoma[J]. Blood, 2023, 141(11): 1293-1307. doi: 10.1182/blood.2022016056
[22] 孙悦, 许宏, 郭振清, 等. 探索18F-FDG PET/CT SUVmax、SUVsum及病理Ki67表达等在非霍奇金淋巴瘤中的临床应用价值[J]. 临床血液学杂志, 2021, 34(1): 18-23. https://lcxy.whuhzzs.com/article/doi/10.13201/j.issn.1004-2806.2021.01.005
[23] Shannon-Lowe C, Rickinson AB, Bell AI. Epstein-Barr virus-associated lymphomas[J]. Philos Trans R Soc Lond B Biol Sci, 2017, 372(1732): 20160271. doi: 10.1098/rstb.2016.0271
[24] Sausen DG, Basith A, Muqeemuddin S. EBV and Lymphomagenesis[J]. Cancers, 2023, 15(7): 2133. doi: 10.3390/cancers15072133
-
图(2)
表(3)
计量
- 文章访问数: 1075
- PDF下载数: 656
- 施引文献: 0