
-
摘要: 目的探讨再生障碍性贫血(AA)患者血清转化生长因子-β(TGF-β)、血小板生成素(TPO)的表达,并分析二者与AA患者病情程度的关系。方法选取2018年12月至2021年12月北部战区总医院收治的128例AA患者作为AA组,另选取同期收治的128例缺铁性贫血患者作为对照组。依据《再生障碍性贫血诊断与治疗中国专家共识(2017版)》中AA病情分型,将AA组患者分为重型组与非重型组;设计患者基线资料调查表,检测患者相关实验室指标,比较AA组与对照组、重型组与非重型组患者基线资料、实验室指标,重点分析血清TGF-β、TPO在AA患者中的表达及其与AA病情分型的关系。结果128例AA患者中重型75例(58.59%),非重型53例(41.41%);AA组患者白细胞计数(WBC)、中性粒细胞绝对值(ANC)、血红蛋白(Hb)、血小板计数(PLT)、网织红细胞绝对值(RET#)、CD4+T淋巴细胞、TGF-β水平显著低于对照组,CD8+T淋巴细胞、TPO水平显著高于对照组(P<0.05)。重型组患者脾、淋巴结肿大占比显著高于非重型组,ANC、PLT、RET#、CD4+T淋巴细胞、TGF-β水平显著低于非重型组,CD8+T淋巴细胞、TPO水平显著高于非重型组(P<0.05)。绘制受试者工作特征曲线,结果显示,TGF-β、TPO单独及联合检测评估AA病情程度的曲线下面积>0.70,具有一定的评估价值;限制性立方样条分析结果显示,血清TGF-β、TPO表达与AA患者病情程度分型的关联强度呈线性剂量反应关系(P<0.05)。结论血清TGF-β、TPO在AA患者中呈异常表达,且与患者病情程度分型有关。Abstract: ObjectiveTo investigate the expression of serum transforming growth factor-β(TGF-β) and thrombopoietin(TPO) in patients with aplastic anemia(AA), and analyze the relationship between them and the severity of AA patients.MethodsA total of 128 AA patients treated in the Northern Theatre General Hospital from December 2018 to December 2021 were selected as AA group. In addition, 128 patients with iron deficiency anemia treated in the hospital during the same period were selected as the control group. According to the AA condition classification in the Chinese Expert Consensus on the Diagnosis and Treatment of Aplastic Enemia(2017 Edition), patients in AA group were divided into severe group and non severe group; designed the baseline data questionnaire of patients, tested relevant laboratory indexes of patients. The baseline data and laboratory indexes of patients in AA group and control group, severe group and non severe group were compared. The expression of serum TGF-β and TPO in AA patients and their relationship with the classification of AA were mainly analyzed.ResultsAmong 128 AA patients, 75 cases(58.59%) were severe and 53 cases(41.41%) were non severe. Compared with the control group, the levels of leukocyte count(WBC), neutrophil absolute value(ANC), hemoglobin(Hb), platelet count(PLT), reticulocyte absolute value(RET#), CD4+T lymphocytes and TGF-β of patients in AA group were significantly lower, while the levels of CD8+T lymphocytes and TPO were significantly higher(P < 0.05).Compared with non severe group, the proportion of splenomegaly and lymphadenopathy of patients in severe group was significantly higher, the levels of ANC, PLT, RET#, CD4+T lymphocytes and TGF-β were significantly lower, and the levels of CD8+T lymphocytes and TPO were significantly higher(P < 0.05).The area under the curve of single and combined detection of TGF-β and TPO in evaluating the severity of AA were>0.70, which had certain evaluation value.There was a linear dose-response relationship between the expression of serum TGF-β and TPO and the severity classification of AA patients(P < 0.05).ConclusionSerum TGF-β and TPO were abnormally expressed in AA patients, which might be related to the degree of disease classification of patients.
-
Key words:
- aplastic anemia /
- severe /
- transforming growth factor-β /
- thrombopoietin
-

-
表 1 AA组与对照组基线资料、实验室指标比较
X±S 项目 AA组(128例) 对照组(128例) t/χ2 P 年龄/岁 62.47±4.55 61.95±4.21 0.949 0.344 性别/例(%) 0.393 0.531 男 66(51.56) 71(55.47) 女 62(48.44) 57(44.53) WBC/(×109·L-1) 2.02±0.64 4.96±1.21 24.300 <0.001 ANC/(×109·L-1) 0.47±0.13 2.25±0.57 34.927 <0.001 Hb/(g·L-1) 56.42±10.18 72.56±12.33 11.420 <0.001 PLT/(×109·L-1) 20.30±5.56 78.63±12.73 51.924 <0.001 RET#/(×109·L-1) 19.07±4.61 26.87±6.38 11.221 <0.001 CD3+/% 67.60±11.16 66.85±10.97 0.542 0.588 CD4+/% 26.99±6.86 31.85±8.24 5.128 <0.001 CD8+/% 34.08±8.63 29.23±7.15 4.897 <0.001 TGF-β/(pg·mL-1) 30.44±6.57 41.34±9.43 10.729 <0.001 TPO/(pg·μL-1) 2.83±0.77 0.78±0.12 30.040 <0.001  下载: 导出CSV
下载: 导出CSV
表 2 重型组与非重型组基线资料比较
X±S 项目 重型组(75例) 非重型组(53例) t/χ2 P 年龄/岁 62.58±4.69 62.31±4.43 0.328 0.743 性别/例(%) 0.699 0.403 男 41(54.67) 25(47.17) 女 34(45.33) 28(52.83) 病程/月 27.62±5.87 26.95±5.64 0.646 0.519 获得因素/例(%) 0.861 0.650 病毒感染 27(36.00) 20(37.74) 免疫异常 31(41.33) 18(33.96) 其他 17(22.67) 15(28.30) 发热/例(%) 2.539 0.111 是 59(78.67) 35(66.04) 否 16(21.33) 18(33.96) 脾肿大/例(%) 4.901 0.027 有 46(61.33) 22(41.51) 无 29(38.67) 31(58.49) 淋巴结肿大/例(%) 4.380 0.036 有 38(50.67) 17(32.08) 无 37(49.33) 36(67.92)
下载: 导出CSV
表 3 重型组与非重型组实验室指标比较
X±S 项目 重型组(75例) 非重型组(53例) χ2 P WBC/(×109·L-1) 1.95±0.53 2.11±0.71 1.460 0.147 ANC/(×109·L-1) 0.43±0.10 0.52±0.14 3.688 <0.001 Hb/(g·L-1) 55.84±9.88 57.23±10.74 0.756 0.451 PLT/(×109·L-1) 18.28±4.95 23.18±5.13 5.432 <0.001 RET#/(×109·L-1) 17.55±3.83 21.24±4.78 4.663 <0.001 CD3+/% 67.88±11.25 67.21±11.04 0.334 0.739 CD4+/% 25.25±6.22 29.43±7.05 3.545 0.001 CD8+/% 35.88±8.77 31.54±7.83 2.881 0.005 TGF-β/(pg·mL-1) 28.46±5.17 33.25±7.33 4.091 <0.001 TPO/(pg·μL-1) 3.06±0.78 2.51±0.62 3.709 <0.001
下载: 导出CSV
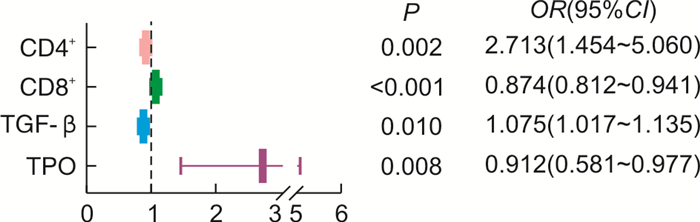
表 4 各因素影响AA患者病情程度的回归分析
相关因素 β SE Wald χ2 P OR 95%CI CD4+ -0.092 0.035 6.949 0.008 0.912 0.851~0.977 CD8+ 0.072 0.028 6.581 0.010 1.075 1.017~1.135 TGF-β -0.134 0.038 12.659 <0.001 0.874 0.812~0.941 TPO 0.998 0.318 9.843 0.002 2.713 1.454~5.060 常量 1.847 1.942 0.905 0.342 - -
下载: 导出CSV
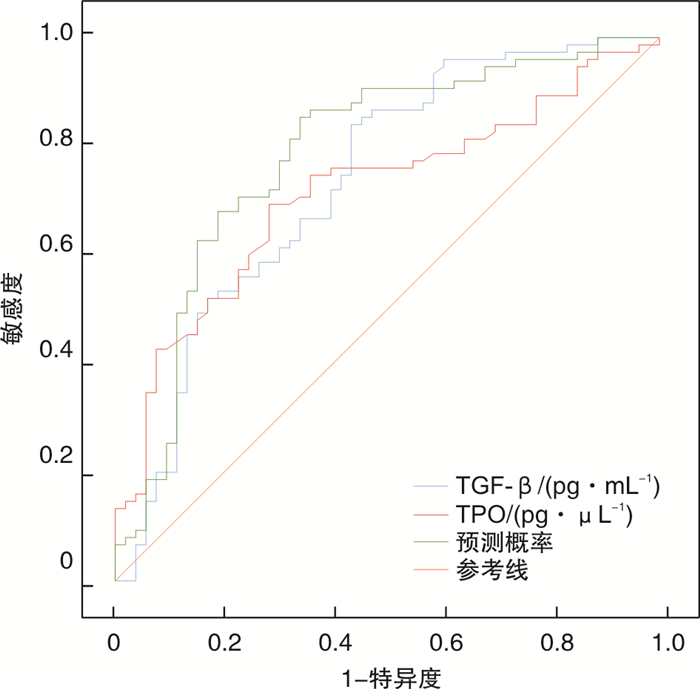
表 5 TGF-β、TPO对AA患者疾病程度分型的评估价值
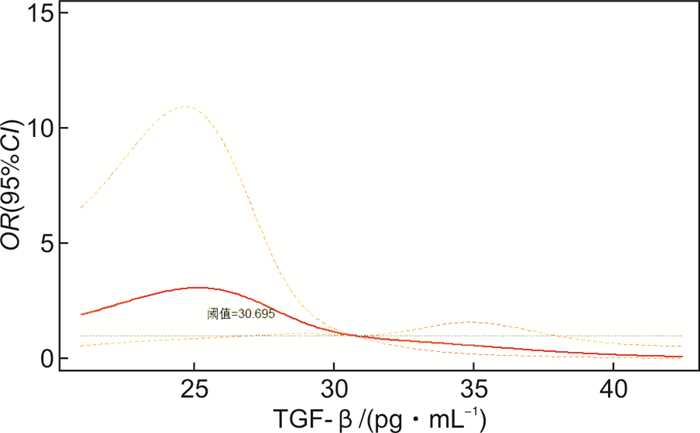
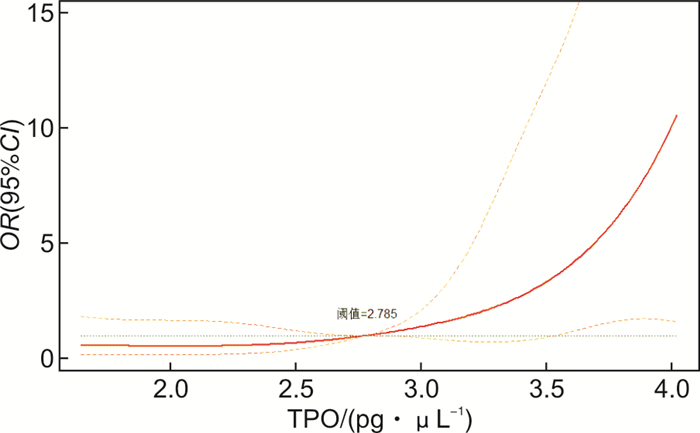
项目 AUC 截断值 95%CI P 特异度 敏感度 Youden TGF-β 0.734 30.695 pg/mL 0.643~0.825 <0.001 0.660 0.667 0.327 TPO 0.714 2.785 pg/μL 0.624~0.803 <0.001 0.717 0.693 0.410 联合 0.785 0.576 0.700~0.870 <0.001 0.717 0.720 0.437
下载: 导出CSV
-
[1] Ye L, Zhang F, Kojima S. Current insights into the treatments of severe aplastic anemia in China[J]. Int J Hematol, 2020, 112(3): 292-299. doi: 10.1007/s12185-020-02955-1
[2] Liu LP, Chen XJ, Yang WY, et al. Predicting response to porcine antilymphocyte globulin plus cyclosporine A in children with acquired severe aplastic anemia[J]. Pediatr Res, 2019, 86(3): 360-364. doi: 10.1038/s41390-019-0437-1
[3] Bewersdorf JP, Zeidan AM. Transforming growth factor(TGF)-β pathway as a therapeutic target in lower risk myelodysplastic syndromes[J]. Leukemia, 2019, 33(6): 1303-1312. doi: 10.1038/s41375-019-0448-2
[4] 褚保凤, 底建辉, 方强, 等. 血清中MRE11、TPO、Th 17Treg、IL-17、VEGF在儿童再生障碍性贫血免疫发病的诊断价值及治疗意义[J]. 中国实验诊断学, 2019, 23(10): 1693-1697. doi: 10.3969/j.issn.1007-4287.2019.10.004
[5] 中华医学会血液学分会红细胞疾病(贫血)学组. 再生障碍性贫血诊断与治疗中国专家共识(2017年版)[J]. 中华血液学杂志, 2017, 38(1): 1-5. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXZ201711001.htm
[6] 中华医学会血液学分会红细胞疾病(贫血)学组. 铁缺乏症和缺铁性贫血诊治和预防多学科专家共识[J]. 中华医学杂志, 2018, 98(28): 2233-2237. doi: 10.3760/cma.j.issn.0376-2491.2018.28.004
[7] 贺锋, 程金凤, 蔡细英. 地中海贫血和再生障碍性贫血患者输注不同Rh抗原匹配红细胞后的血清学特征及疗效[J]. 临床血液学杂志, 2020, 33(8): 541-544. http://lcxz.cbpt.cnki.net/WKC/WebPublication/paperDigest.aspx?paperID=58d2f6b2-751a-467f-b450-079098229792
[8] Xu ZL, Zhou M, Jia JS, et al. Immunosuppressive therapy versus haploidentical transplantation in adults with acquired severe aplastic anemia[J]. Bone Marrow Transplant, 2019, 54(8): 1319-1326. doi: 10.1038/s41409-018-0410-3
[9] Kelaidi C, Makis A, Tzotzola V, et al. Severe aplastic anaemia in children: Impact of histopathology profile and treatment on very long-term outcomes[J]. Acta Paediatr, 2021, 110(4): 1308-1314. doi: 10.1111/apa.15546
[10] 余祖辉. 骨髓细胞学、白细胞、血清铁蛋白联合检查对再生障碍性贫血的诊断价值[J]. 检验医学与临床, 2021, 18(13): 1825-1827, 1832. doi: 10.3969/j.issn.1672-9455.2021.13.001
[11] 唐旭东, 刘锋, 李柳, 等. 血小板计数在以补肾中药为主联合ATG/ALG治疗重型再障的预测作用[J]. 时珍国医国药, 2018, 29(5): 1266-1270. https://www.cnki.com.cn/Article/CJFDTOTAL-SZGY201805085.htm
[12] Babushok DV, Grignon AL, Li Y, et al. Disrupted lymphocyte homeostasis in hepatitis-associated acquired aplastic anemia is associated with short telomeres[J]. Am J Hematol, 2016, 91(2): 243-247. doi: 10.1002/ajh.24256
[13] Matsuda K, Koya J, Arai S, et al. Cyclosporine Therapy in Patients with Transfusion-independent Non-severe Aplastic Anemia: A Retrospective Analysis[J]. Intern Med, 2019, 58(3): 355-360. doi: 10.2169/internalmedicine.1372-18
[14] Velegraki M, Salem M, Ansa-Addo EA, et al. Autocrine transforming growth factor β1 in regulatory T cell biology-gone but not missed[J]. Immunity, 2021, 54(3): 395-396. doi: 10.1016/j.immuni.2021.02.007
[15] Nakamura-Ishizu A, Chin D, Matsumura T, et al. Prolonged maintenance of hematopoietic stem cells that escape from thrombopoietin deprivation[J]. Blood, 2021, 137(19): 2609-2620. doi: 10.1182/blood.2020005517
[16] Cattley RT, Lee M, Boggess WC, et al. Transforming growth factor β(TGF-β)receptor signaling regulates kinase networks and phosphatidylinositol metabolism during T-cell activation[J]. J Biol Chem, 2020, 295(24): 8236-8251. doi: 10.1074/jbc.RA120.012572
[17] Gao L, Cen S, Wang P, et al. Autophagy Improves the Immunosuppression of CD4+ T Cells by Mesenchymal Stem Cells Through Transforming Growth Factor-β1[J]. Stem Cells Transl Med, 2016, 5(11): 1496-1505. doi: 10.5966/sctm.2015-0420
[18] Konkel JE, Zhang D, Zanvit P, et al. Transforming Growth Factor-β Signaling in Regulatory T Cells Controls T Helper-17 Cells and Tissue-Specific Immune Responses[J]. Immunity, 2017, 46(4): 660-674. doi: 10.1016/j.immuni.2017.03.015
[19] 袁长威, 熊媛媛, 张青兰, 等. 标准免疫抑制治疗联合重组人血小板生成素及艾曲波帕治疗重型再生障碍性贫血2例报告及文献复习[J]. 临床血液学杂志, 2020, 33(7): 503-507. http://lcxz.cbpt.cnki.net/WKC/WebPublication/paperDigest.aspx?paperID=34ad8628-8561-4da3-a31e-6eaa29e01ec5
[20] Corey SJ. The Highs and Lows of Measuring Thrombopoietin in Aplastic Anemia[J]. Pediatr Blood Cancer, 2016, 63(4): 585-586.
[21] Zhao X, Feng X, Wu Z, et al. Persistent elevation of plasma thrombopoietin levels after treatment in severe aplastic anemia[J]. Exp Hematol, 2018, 58: 39-43.
-
图(4)
表(5)
计量
- 文章访问数: 751
- PDF下载数: 233
- 施引文献: 0