
Analysis of predictive factors for hematopoietic stem cell mobilization by plerixafor plus G-CSF in patients with multiple myeloma
-
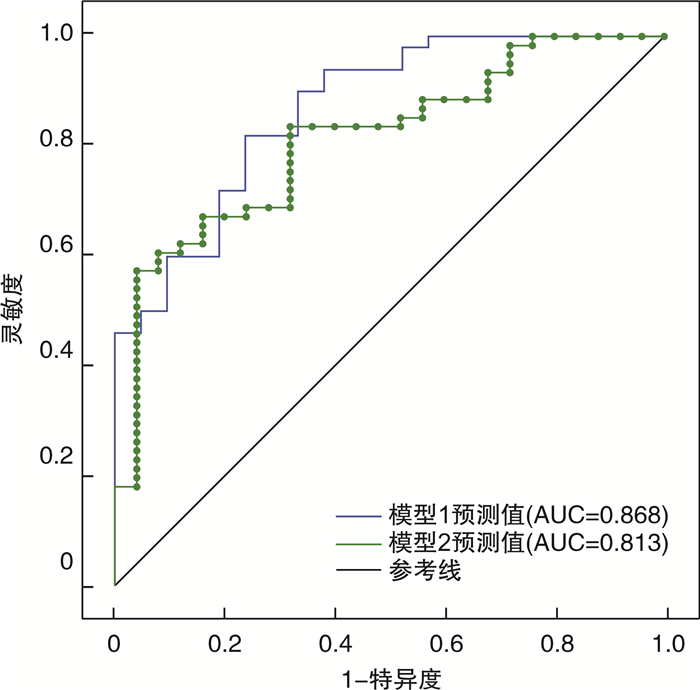
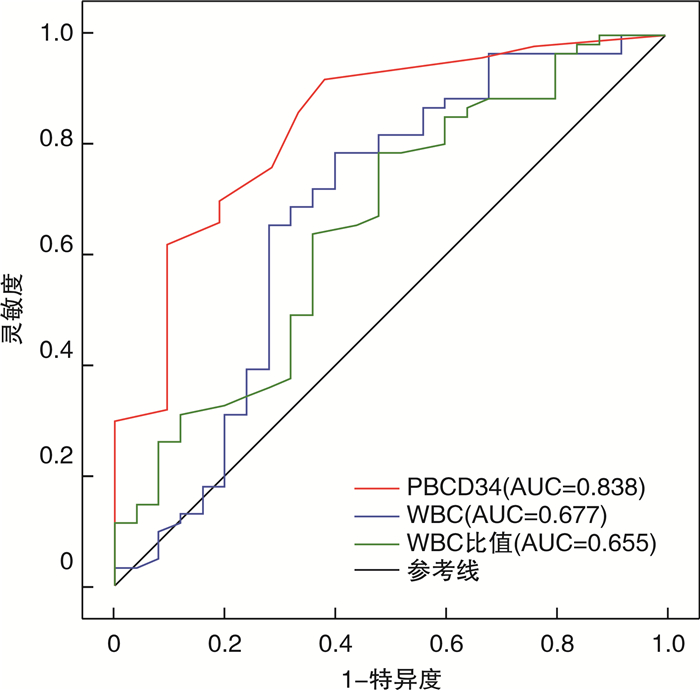
摘要: 目的 探讨多发性骨髓瘤(multiple myeloma,MM)患者普乐沙福动员自体外周血造血干细胞的影响因素。方法 收集浙江大学医学院附属第一医院骨髓移植中心2018年8月—2021年10月接受普乐沙福联合粒细胞集落刺激因子(granulocyte colony-stimulating factor,G-CSF)动员外周血造血干细胞的86例MM患者数据,分析年龄、体重、BMI、既往化疗、既往放疗、基础疾病、动员前疾病状态、动员前基线外周血细胞水平、普乐沙福应用前后(即采集第-1天和采集第1天)外周血各类细胞水平等因素,探讨这些因素对普乐沙福首次动员效率的影响。结果 患者中位年龄57(38~67)岁,中位采集天数2(1~4) d。首次采集成功率为70.9%,动员成功率为88.4%。单因素分析中ISS分期、糖尿病、第-1天外周血CD34+细胞计数(PBCD34)、第1天WBC、第1天/第-1天WBC比(WBC比值)差异有统计学意义(P<0.05)。多因素logistic回归分析模型1中,第-1天PBCD34(OR=1.299,95%CI 1.12~1.51,P=0.001)和ISS分期(OR=0.159,95%CI 0.03~0.90,P=0.037)差异有统计学意义。模型2中第1天WBC(OR=1.037,95%CI 1.00~1.07,P=0.043),WBC比值(OR=7.553,95%CI 1.06~53.76,P=0.043)和ISS分期(OR=0.112,95%CI 0.03~0.49,P=0.004)差异有统计学意义。结论 单因素分析中ISSⅢ期、合并糖尿病、第-1天PBCD34 < 3.5/μL、第1天WBC < 38×109/L、WBC比值< 1.4是首次采集的不良影响因素。在多因素分析预测模型中,第-1天PBCD34仍是动员的独立预测因素。Abstract: Objective To identify the factors associated with autologous peripheral blood hematopoietic stem cell (HSC) mobilization after plerixafor administration in patients with multiple myeloma (MM).Methods A retrospective analysis of 86 patients with newly diagnosed MM who received plerixafor combined with granulocyte colony-stimulating factor(G-CSF) to mobilize HSC from August 2018 to October 2021 was performed in the Bone Marrow Transplantation Center of the First Affiliated Hospital of Zhejiang University School of Medicine. The factors, such as body weight, BMI, previous chemotherapy regimen, previous radiotherapy, comorbidities, disease status before mobilization, baseline peripheral blood cell level before mobilization, and peripheral blood cell level before and after plerixafor administration(day-1 and day 1 of apheresis), were analyzed to explore the influence on the mobilization efficiency of plerixafor.Results The median age was 57(38-67) years. The median apheresis days were 2(1-4) days. In univariate analysis, ISS stage, diabetes, peripheral blood CD34+cell count on day-1(day-1 PBCD34), day 1 WBC count, and the ratio of day 1 WBC count /day-1 WBC count before mobilization(WBC ratio) were statistically significant(P < 0.05). In multivariate logistic regression analysis model 1, day-1 PBCD34(OR=1.299, 95%CI 1.12-1.51, P=0.001) and ISS stage(OR=0.159, 95%CI 0.03-0.90, P=0.037) has statistical significance. In model 2, statistically significant associations were observed in day 1 WBC count(OR=1.037, 95%CI 1.00-1.07, P=0.043), WBC ratio(OR=7.553, 95%CI 1.06-53.76, P=0.043), and ISS stage(OR=0.112, 95%CI 0.03-0.49, P=0.004).Conclusion In univariate analysis, ISS stage Ⅲ, diabetes, day-1 PBCD34 < 3.5/μL, day 1 WBC count < 38×109/L, and WBC ratio < 1.4 were risk factors of poor mobilization on first leukaphereses. In multivariate analysis prediction model, day-1 PBCD34 was still an independent predictor of mobilization.
-

-
表 1 患者基线特征
特征 首次采集成功组(n=61) 首次采集失败组(n=25) P 年龄/岁 56.0±5.8 54.8±8.7 0.905 性别/例(%) 0.668 男 36(59.0) 16(64.0) 女 25(41.0) 9(36.0) 体重/kg 65.0(57.5,71.0) 66.0(59.3,71.5) 0.905 BMI 24.0±3.1 24.8±2.6 0.905 DS分期/例(%) 0.818 Ⅰ 3(4.9) 0 Ⅱ 13(21.3) 5(20.0) Ⅲ 43(70.5) 20(80.0) 缺失 2(3.3) 0 ISS分期/例(%) 0.009 Ⅰ* 25(41.0) 4(16.0) Ⅱ 19(31.1) 6(24.0) Ⅲ 12(19.7) 14(56.0) 缺失 5(8.2) 1(4.0) 疗程数/个 4(3~10) 4(3~11) 0.665 治疗线数 1(1~3) 1(1~3) 0.665 来那度胺/例(%) 38(62.3) 18(72.0) 0.391 单药疗程数/个 硼替佐米 4(2~9) 4(3~11) 0.467 环磷酰胺 0(0~7) 1(0~5) 0.193 来那度胺 2(0~5) 3(0~6) 0.384 沙利度胺 0(0~5) 0(0~2) 0.748 伊沙佐米 0(0~2) 0(0~1) 0.362 阿霉素 0(0~3) 0(0~4) 0.653 达雷妥尤单抗 0(0~8) 0(0~9) 0.078 缓解状态/例(%) 0.148 CR 22(36.1) 9(36.0) VGPR 28(45.9) 15(60.0) PR 11(18.0) 1(4.0) MRD阴性/例(%) 43(70.5) 20(80.0) 0.366 动员前基线外周血计数/(×109/L) WBC 5.3±1.6 4.8±1.6 0.328 HB 123.7±18.8 117.8±19.5 0.101 PLT 208.0(162.0,255.0) 198.0(151.5,246.5) 0.427 MNC 0.4(0.3,0.6) 0.4(0.3,0.5) 0.973 其他 游离轻链比值 0.9(0.7,1.6) 1.0(0.3,1.4) 0.396 骨髓浆细胞比例/% 0(0~5.0) 0(0~3.0) 0.500 乳酸脱氢酶/(U/L) 209.0(179.0,252.0) 194.0(169.5,209.0) 0.314 球蛋白/(g/L) 21.0(18.8,22.6) 19.6(18.0,22.4) 0.168 甘油三酯/(mmol/L) 1.5(1.2,2.4) 1.4(1.2,1.9) 0.300 白蛋白/(g/L) 43.4±2.63 41.9±3.1 0.251 总胆固醇/(mmol/L) 5.0±0.9 4.9±1.3 0.486 伴随疾病/例(%) 肾功能不全 11(18.0) 5(20.0) 0.831 糖尿病 3(4.9) 6(24.0) 0.025 高血压 12(19.7) 4(16.0) 0.927 脂肪肝 18(30.0) 5(20.0) 0.344 *ISS Ⅰ期为对照组。  下载: 导出CSV
下载: 导出CSV
表 2 患者治疗特征
特征 首次采集成功组(n=61) 首次采集失败组(n=25) P 第-1天外周血细胞计数/(×109/L) WBC 30.6(25.3,43.4) 26.0(19.3,35.6) 0.189 HB 119.0±16.0 110.0±16.7 0.101 PLT 170.0(132.0,202.0) 152.5(115.5,213.5) 0.142 MNC 2.0±0.8 2.1±0.7 0.438 第1天外周血细胞计数/(×109/L) WBC 51.2±15.8 44.7±19.1 0.016 HB 123.5±14.6 117.4±16.0 0.147 PLT 179.0(135.0,207.5) 151.0(127.5,207.0) 0.077 MNC 4.9±1.5 4.4±1.6 0.074 第1天/第-1天外周血细胞比 WBC 1.6(1.4,1.7) 1.4(1.3,1.7) 0.025 HB 1.0±0.1 1.0±0.05 0.456 PLT 1.0±0.1 1.0±0.1 0.439 MNC 2.4(2.0,3.0) 2.4(1.6,2.8) 0.268 普乐沙福用法/例(%) 0.353 临床试验组 10(16.4) 7(28.0) 真实世界组 51(83.6) 18(72.0) 第-1天PBCD34/μL 11.0(1.0~65.0) 3.0(1.0~16.0) < 0.001 第1天PBCD34/μL 59.0(17.0~175.0) 11.5(3.0~40.0) < 0.001 第1天CD34+细胞计数/(×106/L) 3.7(2.1~12.2) 1.0(0.1~1.7) < 0.001 总CD34+细胞计数/(×106/L) 6.2±2.0 2.4±1.4 < 0.001
下载: 导出CSV
表 3 相关系数矩阵
临床特征 WBCa PLTa MNCa PBCD34a WBC比值 Dara 糖尿病 ISS分期 PLTa 0.5731) MNa 0.5361) 0.4711) PBCD34a 0.4671) 0.199 0.2811) WBC比值 0.182 0.048 0.130 0.3121) Dara -0.088 -0.185 -0.059 -0.093 -0.203 糖尿病 -0.2471) 0.076 -0.093 -0.027 -0.125 0.040 ISS分期 0.081 0.141 0.037 -0.052 0.085 0.121 0.096 首次采集CD34+细胞数 0.3821) 0.2931) 0.206 0.6421) 0.5191) -0.2241) -0.2381) -0.171 aWBC/PLT/MNC/PBCD34均为第1天外周血细胞计数;1)P < 0.05。
下载: 导出CSV
-
[1] Cowan AJ, Green DJ, Kwok M, et al. Diagnosis and management of multiple myeloma: areview[J]. JAMA, 2022, 327(5): 464-477. doi: 10.1001/jama.2022.0003
[2] Ntanasis-Stathopoulos I, Gavriatopoulou M, Kastritis E, et al. Multiple myeloma: role of autologous transplantation[J]. Cancer Treat Rev, 2020, 82: 101929. doi: 10.1016/j.ctrv.2019.101929
[3] Dhakal B, Szabo A, Chhabra S, et al. Autologous transplantation for newly diagnosed multiple myeloma in the era of novel agent induction: asystematic review and meta-analysis[J]. JAMA Oncol, 2018, 4(3): 343-350. doi: 10.1001/jamaoncol.2017.4600
[4] 李娟, 刘俊茹. 自体造血干细胞移植在多发性骨髓瘤治疗中的优化和生存趋势[J]. 临床血液学杂志, 2021, 34(7): 449-453. doi: 10.13201/j.issn.1004-2806.2021.07.001
[5] Wang JZ, Tannous BA, Poznansky MC, et al. CXCR4 antagonist AMD3100(plerixafor): from an impurity to a therapeutic agent[J]. Pharmacol Res, 2020, 159: 105010. doi: 10.1016/j.phrs.2020.105010
[6] DiPersio JF, Stadtmauer EA, Nademanee A, et al. Plerixafor and G-CSF versus placebo and G-CSF to mobilize hematopoietic stem cells for autologous stem cell transplantation in patients with multiple myeloma[J]. Blood, 2009, 113(23): 5720-5726. doi: 10.1182/blood-2008-08-174946
[7] Lazzaro C, Castagna L, Lanza F, et al. Chemotherapy-based versus chemotherapy-free stem cell mobilization(±plerixafor)in multiple myeloma patients: an Italian cost-effectiveness analysis[J]. Bone Marrow Transplant, 2021, 56(8): 1876-1887. doi: 10.1038/s41409-021-01251-8
[8] Johnsrud A, Ladha A, Muffly L, et al. Stem cell mobilization in multiple myeloma: comparing safety and efficacy of cyclophosphamide +/- plerixafor versus granulocyte colony-stimulating factor +/- plerixafor in the lenalidomide era[J]. Transplant Cell Ther, 2021, 27(7): 590. e1-590. e8. doi: 10.1016/j.jtct.2021.04.016
[9] Fergadis E, Assi A, Kranidioti E, et al. Plerixafor-aided mobilization of peripheral blood hematopoietic stem cells to support subsequent high-dose chemotherapy after a prior autologous transplant[J]. Clin Lymphoma Myeloma Leuk, 2020, 20(2): e50-e57. doi: 10.1016/j.clml.2019.11.022
[10] Swinn T, Butler A. Plerixafor use in New Zealand 2016-2019: an observational study[J]. Intern Med J, 2022 May 13. doi:
10.1111/imj.15819.Epubaheadofprint .[11] Dogu MH, Batgi H, Erkurt MA, et al. Stem cell mobilization kinetics in elderly patients with multiple myeloma[J]. Transfus Apher Sci, 2018, 57(2): 204-207. doi: 10.1016/j.transci.2018.01.010
[12] Zheng GF, He JS, Cai Z, et al. A retrospective study of autologous stem cell mobilization by G-CSF in combination with chemotherapy in patients with multiple myeloma and lymphoma[J]. Oncol Lett, 2020, 19(1): 1051-1059.
[13] Fadini GP, DiPersio JF. Diabetes mellitus as a poor mobilizer condition[J]. Blood Rev, 2018, 32(3): 184-191. doi: 10.1016/j.blre.2017.11.002
[14] Mohty M, Hübel K, Kröger N, et al. Autologous haematopoietic stem cell mobilisation in multiple myeloma and lymphoma patients: a position statement from the European Group for Blood and Marrow Transplantation[J]. Bone Marrow Transplant, 2014, 49(7): 865-872. doi: 10.1038/bmt.2014.39
[15] Wallington-Beddoe CT, Mynott RL. Prognostic and predictive biomarker developments in multiple myeloma[J]. J Hematol Oncol, 2021, 14(1): 151. doi: 10.1186/s13045-021-01162-7
[16] Başcı S, Yiǧenoǧlu TN, Yaman S, et al. Does myeloma genetic have an effect on stem cell mobilization?[J]. Transfus Apher Sci, 2021, 60(6): 103249. doi: 10.1016/j.transci.2021.103249
[17] Paripati H, Stewart AK, Cabou S, et al. Compromised stem cell mobilization following induction therapy with lenalidomide in myeloma[J]. Leukemia, 2008, 22(6): 1282-1284. doi: 10.1038/sj.leu.2405100
[18] Rybinski B, Rapoport AP, Badros AZ, et al. Prolonged lenalidomide induction does not significantly impair stem cell collection in multiple myeloma patients mobilized with cyclophosphamide or plerixafor: areport from the covid era[J]. Clin Lymphoma Myeloma Leuk, 2022, 22(8): e716-e729. doi: 10.1016/j.clml.2022.03.013
[19] Ma X, Wong SW, Zhou P, et al. Daratumumab binds to mobilized CD34+ cells of myeloma patientsin vitrowithout cytotoxicity or impaired progenitor cell growth[J]. Exp Hematol Oncol, 2018, 7: 27. doi: 10.1186/s40164-018-0119-4
[20] Moreau P, Hulin C, Perrot A, et al. Maintenance with daratumumab or observation following treatment with bortezomib, thalidomide, and dexamethasone with or without daratumumab and autologous stem-cell transplant in patients with newly diagnosed multiple myeloma(CASSIOPEIA): an open-label, randomised, phase 3 trial[J]. Lancet Oncol, 2021, 22(10): 1378-1390. doi: 10.1016/S1470-2045(21)00428-9
[21] Cyrille H, Fritz O, Philippe M, et al. Stem cell yield and transplantation in transplant-eligible newly diagnosed multiple myeloma patients receiving daratumumab + bortezomib/thalidomide/dexamethasone in the phase 3 CASSIOPEIA study[J]. Haematologica, 2021: 106(8): 2257-2260.
[22] Eleutherakis PE, Terpos E, Kanellias N, et al. Impact of daratumumab-containing induction on stem cell mobilization and collection, engraftment and hospitalization parameters among multiple myeloma patients undergoing autologous stem cell transplantation[J]. Blood, 2021, 138: 3886. doi: 10.1182/blood-2021-149499
[23] Chhabra S, Callander NS, Costa LJ, et al. Stem cell collection with daratumumab(DARA)-based regimens in transplant-eligible newly diagnosed multiple myeloma(NDMM)patients(pts)in the griffin and master studies[J]. Blood, 2021, 138(Supplement 1): 2852. doi: 10.1182/blood-2021-149028
[24] Fadini GP, Albiero M. Impaired hematopoietic stem/progenitor cell traffic and multi-organ damage in diabetes[J]. Stem Cells, 2022, 40(8): 716-723. doi: 10.1093/stmcls/sxac035
[25] Albiero M, Fadini GP. Pharmacologic targeting of the diabetic stem cell mobilopathy[J]. Pharmacol Res, 2018, 135: 18-24. doi: 10.1016/j.phrs.2018.07.017
[26] Ferraro F, Lymperi S, Méndez-Ferrer S, et al. Diabetes impairs hematopoietic stem cell mobilization by altering niche function[J]. Sci Transl Med, 2011, 3(104): 104ra101.
[27] 中华医学会血液学分会浆细胞疾病学组, 中国医师协会多发性骨髓瘤专业委员会, 黄晓军, 等. 中国多发性骨髓瘤自体造血干细胞移植指南(2021年版)[J]. 中华血液学杂志, 2021, 42(5): 353-357.
[28] Goker H, Ciftciler R, Demiroglu H, et al. Predictive factors for stem cell mobilization failure in multiple myeloma patients: a single center experience[J]. Transfus Apher Sci, 2020, 59(1): 102595. doi: 10.1016/j.transci.2019.06.023
[29] Ishii A, Jo T, Arai Y, et al. Development of a quantitative prediction model for peripheral blood stem cell collection yield in the plerixafor era[J]. Cytotherapy, 2022, 24(1): 49-58. doi: 10.1016/j.jcyt.2021.09.004
-
图(2)
表(3)
计量
- 文章访问数: 768
- PDF下载数: 210
- 施引文献: 0