
Study on prognostic value of inflammation markers and CD4+/CD8+ ratio in newly diagnosed multiple myeloma patients
-
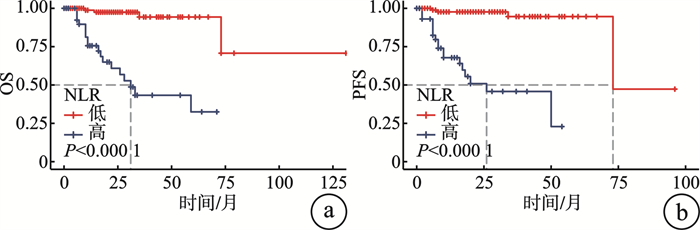
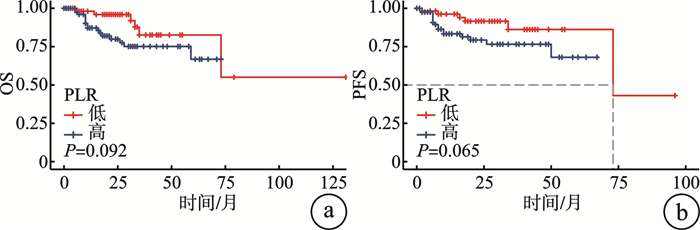
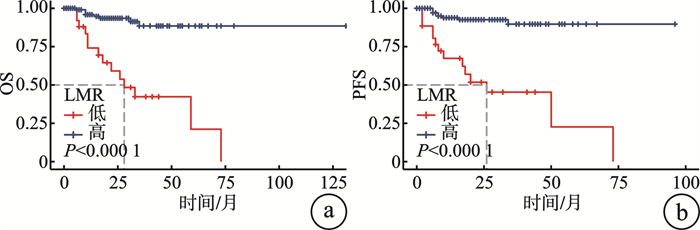
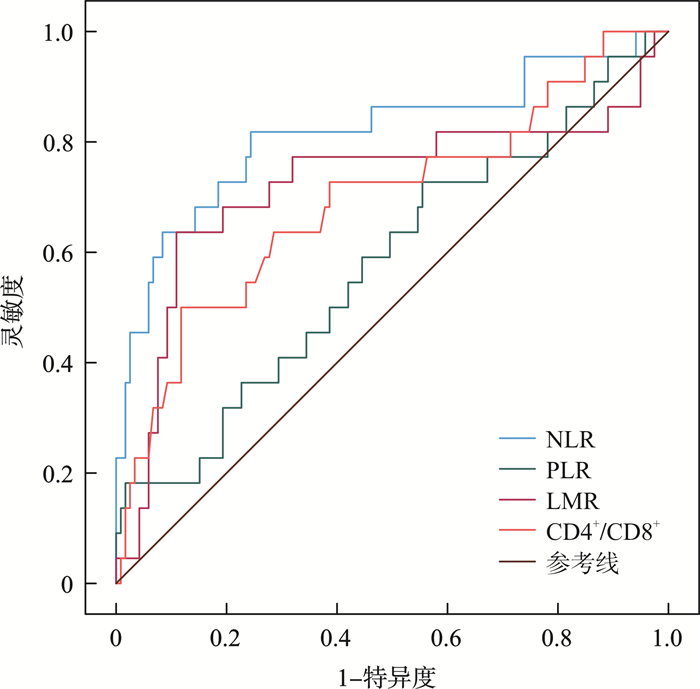
摘要: 目的 分析新诊断多发性骨髓瘤(newly diagnosed multiple myeloma,NDMM)患者的临床特征并探究中性粒细胞与淋巴细胞比(NLR)、血小板-淋巴细胞比(PLR)、淋巴细胞-单核细胞比(LMR)、CD4+/CD8+对于NDMM患者预后的影响。方法 回顾性分析2013年1月—2023年12月就诊于兰州大学第一医院的141例NDMM患者的临床资料,收集其一般资料、临床特征、辅助检查、诊断治疗及疗效预后并计算NLR、PLR、LMR、CD4+/CD8+。结果 通过受试者工作特征(ROC)曲线分别计算出最佳截断值(NLR:2.143,PLR:85.236,LMR:2.584,CD4+/CD8+:0.780),根据此数据分为高NLR组、低NLR组,高PLR组、低PLR组,高LMR组、低LMR组,高CD4+/CD8+组、低CD4+/CD8+组,并与临床资料比较,得到血钙(Ca2+)及乳酸脱氢酶(LDH)对于NLR存在影响(P < 0.05);β2微球蛋白(β2-MG)对于PLR存在影响(P < 0.05);年龄、血小板计数(PLT)、Ca2+、LDH、β2-MG、FISH检测是否异常对于LMR存在影响(P < 0.05);PLT、肌酐(Cr)、Ca2+、FISH检测是否异常对于CD4+/CD8+存在影响。治疗效果数据显示,与高NLR组患者相比,低NLR组患者治疗成效明显更为优秀。多因素分析显示,在NDMM患者中,年龄以及NLR被证实是与总生存期和无进展生存期预后显著相关的独立危险因素(P < 0.05)。结论 NLR、LMR、CD4+/CD8+对于预测NDMM患者预后有重要意义。
-
关键词:
- 新诊断多发性骨髓瘤 /
- 临床特征 /
- 中性粒细胞与淋巴细胞比 /
- CD4+/CD8+
Abstract: Objective To analyze the clinical characteristics of newly diagnosed multiple myeloma(NDMM) patients and explore the effects of neutrophil to lymphocyte ratio(NLR), platelet to lymphocyte ratio(PLR), lymphocyte to monocyte ratio(LMR), and CD4+/CD8+ on prognosis.Methods A retrospective analysis was conducted on the clinical data of 141 NDMM patients in the First Hospital of Lanzhou University from January 2013 to December 2023. General information, clinical characteristics, auxiliary examinations, diagnosis, treatment, and prognosis were collected, and NLR, PLR, LMR, CD4+/CD8+ were calculated.Results The optimal cut-off values(NLR: 2.143, PLR: 85.236, LMR: 2.584, CD4+/CD8+: 0.780) divided patients into high and low groups(high NLR group, low NLR group, high PLR group, low PLR group, high LMR group, low LMR group, high CD4+/CD8+ group, low CD4+/CD8+ group), and by comparing with clinical data, it was found that blood calcium(Ca2+) and lactate dehydrogenase(LDH) levels have an impact on NLR(P < 0.05); β2-MG level has an impact on PLR(P < 0.05); Whether age, platelet count(PLT), Ca2+, LDH, β2-MG, and FISH detection are abnormal have an impact on LMR(P < 0.05); Abnormalities in PLT, creatinine(Cr), Ca2+, and FISH detection have an impact on CD4+/CD8+. The treatment efficacy data shows that patients in the low NLR group have significantly better treatment outcomes compared with patients in the high NLR group. Multivariate analysis showed that age and NLR were significantly independent risk factors associated with overall survival and progression free survival in NDMM patients(P < 0.05).Conclusion NLR, LMR, CD4+/CD8+ are of great significance in predicting the prognosis of NDMM patients. -

-
表 1 NDMM患者临床资料
临床资料 例数(%) 临床资料 例数(%) 年龄 M蛋白类型 < 65岁 77(54.6) IgG型 76(53.9) ≥65岁 64(45.4) IgA型 36(25.5) 性别 轻链型 21(14.9) 男 77(54.6) IgD型 6(4.3) 女 64(45.4) 不分泌型 1(0.7) Hb < 100 g/L 95(67.4) IgM型 1(0.7) PLT < 100×109/L 45(31.9) ISS分期 Cr≥177 μmol/L 26(18.4) Ⅰ期 18(12.8) Ca2+≥2.75 mmol/L 21(14.9) Ⅱ期 48(34.0) β2-MG≥5.5 mg/L 70(49.6) Ⅲ期 75(53.2) UA≥420 μmol/L 58(41.1) BMPC LDH≥250 U/L 27(19.1) < 30% 42(29.8) 髓外病变 10(7.1) ≥30% 99(70.2) 注:Hb:血红蛋白;UA:尿酸;PLT:血小板计数;Cr:肌酐。  下载: 导出CSV
下载: 导出CSV
表 2 NLR、PLR、LMR、CD4+/CD8+水平与临床资料之间的关系
例 临床资料 NLR PLR LMR CD4+/CD8+ < 2.143 ≥2.143 P < 85.236 ≥85.236 P < 2.584 ≥2.584 P < 0.780 ≥0.780 P 年龄/岁 0.108 0.340 0.007 0.773 < 65 56 21 25 42 21 56 13 64 ≥65 38 26 24 40 6 58 12 52 性别 0.120 0.940 0.453 0.298 男 47 30 32 45 13 64 16 61 女 47 17 27 37 14 50 9 55 ISS分期 0.152 0.090 0.258 0.566 Ⅰ/Ⅱ期 48 18 20 46 10 56 13 53 Ⅲ期 46 29 39 36 17 58 12 63 Hb/(g/L) 0.899 0.122 0.200 0.311 < 100 63 32 44 51 21 74 19 76 ≥100 31 15 15 31 6 40 6 40 PLT(×109/L) 0.125 < 0.001 0.003 0.004 < 100 26 19 30 15 15 30 14 31 ≥100 68 28 29 67 12 84 11 85 Cr/(μmol/L) 0.125 0.351 0.095 0.049 < 177 80 35 46 69 19 95 17 98 ≥177 14 12 13 13 8 18 8 18 UA/(μmol/L) 0.090 0.101 0.090 0.224 < 420 60 23 30 53 12 71 12 71 ≥420 34 24 29 29 15 43 13 45 Ca2+/(mmol/L) 0.045 0.561 0.017 0.001 < 2.75 84 33 48 71 19 101 15 105 ≥2.75 10 14 10 11 8 13 10 11 LDH/(U/L) 0.023 0.761 0.002 0.215 < 250 81 33 47 67 16 98 18 96 ≥250 13 14 12 15 11 16 7 20 β2-MG/(mg/L) 0.190 0.008 0.017 0.795 < 5.5 51 20 22 49 8 63 12 59 ≥5.5 43 27 37 33 19 51 13 57 FISH 0.404 0.099 0.039 0.021 正常 52 23 36 39 9 66 8 66 异常 42 24 23 43 17 49 17 50
下载: 导出CSV
表 3 不同NLR、PLR、LMR、CD4+/CD8+水平与临床疗效之间的关系
例 分组 有效 无效 χ2 P 低NLR组 73 21 15.335 < 0.001 高NLR组 21 26 低PLR组 44 15 2.856 0.091 高PLR组 50 32 低LMR组 23 15 3.298 0.069 高LMR组 71 32 低CD4+/CD8+组 13 12 2.942 0.086 高CD4+/CD8+组 81 35
下载: 导出CSV
表 4 影响OS、PFS危险因素的单因素分析
影响因素 OS PFS 95%CI P 95%CI P 性别 0.142~0.993 0.028 0.154~1.032 0.058 年龄 1.594~10.547 0.002 1.716~12.903 0.003 ISS分期 1.268~8.411 0.014 1.369~10.269 0.010 Hb 1.286~8.411 0.011 0.044~0.807 0.025 PLT 0.034~0.298 < 0.001 0.035~0.308 < 0.001 NLR 5.273~61.278 < 0.001 5.992~70.649 < 0.001 PLR 0.856~5.740 0.093 0.909~6.793 0.066 LMR 0.050~0.284 < 0.001 0.049~0.282 < 0.001 Cr 1.265~7.575 0.009 1.202~7.012 0.018 UA 1.263~7.673 0.009 1.269~7.798 0.013 Ca2+ 2.643~14.237 < 0.001 3.232~18.870 < 0.001 LDH 1.890~10.505 0.001 1.800~9.995 0.001 β2-MG 1.339~9.848 0.011 1.304~9.597 0.013 CD4+/CD8+ 0.101~0.539 0.001 0.087~0.486 < 0.001 FISH 1.758~20.380 0.004 2.103~24.310 0.002
下载: 导出CSV
表 5 影响OS、PFS危险因素的多因素分析
影响因素 OS PFS 95%CI P 95%CI P 性别 0.276~4.909 0.835 年龄 1.772~40.003 0.007 1.708~40.232 0.009 ISS分期 0.151~3.474 0.687 0.549~11.831 0.223 Hb 0.053~6.157 0.646 0.061~3.228 0.422 PLT 0.020~0.506 0.005 0.025~0.668 0.012 NLR 2.098~74.782 0.006 1.571~41.298 0.012 LMR 0.134~1.813 0.287 0.099~1.303 0.360 Cr 0.793~8.353 0.115 0.804~6.903 0.118 UA 0.138~2.400 0.449 0.216~2.8 968 0.724 Ca2+ 0.483~3.868 0.556 0.356~3.980 0.777 LDH 0.299~3.225 0.977 0.299~3.061 0.942 β2-MG 0.166~6.383 0.976 0.066~2.298 0.298 CD4+/CD8+ 0.108~1.557 0.190 0.101~1.438 0.155 FISH 0.440~16.482 0.284 0.622~10.781 0.191
下载: 导出CSV
-
[1] Shieh AC, Faraji N, Smith D, et al. Utility and Clinical Implications of Appendicular Skeleton Magnetic Resonance Imaging in Multiple Myeloma: A Single-Institutional 15-Year Experience[J]. J Comput Assist Tomogr, 2021, 45(6): 904-911. doi: 10.1097/RCT.0000000000001195
[2] Szlasa W, Dybko J. Current status of bispecific antibodies and CAR-T therapies in multiple myeloma[J]. Int Immunopharmacol, 2024, 134: 112043. doi: 10.1016/j.intimp.2024.112043
[3] Bergsagel PL. Where we were, where we are, where we are going: progress in multiple myeloma[J]. Am Soc Clin Oncol Educ Book, 2014, 34(1): 199-203.
[4] Zhang X, Duan J, Wen Z, et al. Are the Derived Indexes of Peripheral Whole Blood Cell Counts(NLR, PLR, LMR/MLR)Clinically Significant Prognostic Biomarkers in Multiple Myeloma?A Systematic Review And Meta-Analysis[J]. Front Oncol, 2021, 11: 766672. doi: 10.3389/fonc.2021.766672
[5] Rajkumar SV, Dimopoulos MA, Palumbo A, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma[J]. Lancet Oncol, 2014, 15(12): e538-e548. doi: 10.1016/S1470-2045(14)70442-5
[6] 杜鹃, 侯健. 《中国多发性骨髓瘤诊治指南》2022年修订诊断部分解读[J]. 中华内科杂志, 2022, 61(5): 463-465. doi: 10.3760/cma.j.cn112138-20220316-00182
[7] Hu H, Cheng R, Wang Y, et al. Oncogenic KRAS signaling drives evasion of innate immune surveillance in lung adenocarcinoma by activating CD47[J]. J Clin Invest, 2023, 133(2): e153470. doi: 10.1172/JCI153470
[8] Hájek R, Krejcí M, Pour L, et al. Multiple myeloma[J]. Klin Onkol, 2011, 24(Suppl): S10-S13.
[9] Radhakrishnan V, Golla U, Kudva AK. Role of Immune Cells and Immunotherapy in Multiple Myeloma[J]. Life(Basel), 2024, 14(4): 461.
[10] Moscvin M, Evans B, Bianchi G. Dissecting molecular mechanisms of immune microenvironment dysfunction in multiple myeloma and precursor conditions[J]. J Cancer Metastasis Treat, 2023, 9: 17.
[11] Malek E, de Lima M, Letterio JJ, et al. Myeloid-derived suppressor cells: The green light for myeloma immune escape[J]. Blood Rev, 2016, 30(5): 341-348. doi: 10.1016/j.blre.2016.04.002
[12] Li S, Lu Z, Wu S, et al. The dynamic role of platelets in cancer progression and their therapeutic implications[J]. Nat Rev Cancer, 2024, 24(1): 72-87. doi: 10.1038/s41568-023-00639-6
[13] Chen L, Zhu C, Pan F, et al. Platelets in the tumor microenvironment and their biological effects on cancer hallmarks[J]. Front Oncol, 2023, 13: 1121401. doi: 10.3389/fonc.2023.1121401
[14] Chen S, Zhou M, Yang J, et al. Significance of Common Blood Test Indexes in the Diagnosis and Prognosis of Multiple Myeloma[J]. Clin Lab, 2022, 68(4).
[15] Raja MRK, Gupta G, Atkinson G, et al. Host-derived Interleukin 1α induces an immunosuppressive tumor microenvironment via regulating monocyte-to-macrophage differentiation [J]. bioRxiv, 2024: 2024.05.03.592354.
[16] Morè S, Corvatta L, Manieri MV, et al. Real-world assessment of treatment patterns and outcomes in patients with relapsed-refractory multiple myeloma in an Italian haematological tertiary care centre[J]. Br J Haematol, 2023, 201(3): 432-442. doi: 10.1111/bjh.18658
[17] 杨植然, 刘文博, 刘庆伟, 等. 肿瘤相关巨噬细胞脂质代谢重编程与胃肠道肿瘤靶向治疗策略研究进展[J]. 肿瘤学杂志, 2024, 30(8): 630-636.
[18] Huang H, Li L, Luo W, et al. Lymphocyte percentage as a valuable predictor of prognosis in lung cancer[J]. J Cell Mol Med, 2022, 26(7): 1918-1931. doi: 10.1111/jcmm.17214
[19] 陈娟, 石志, 娄慧娟, 等. 系统免疫-炎症指数对初诊多发性骨髓瘤患者预后的评估价值[J]. 临床血液学杂志, 2022, 35(3): 180-186. https://lcxy.whuhzzs.com/article/doi/10.13201/j.issn.1004-2806.2022.03.006
[20] 王跃飞, 陈葆国, 郑瑞, 等. PD-1/PD-L1在MDS原始细胞、T细胞亚群和Treg细胞中的表达及意义[J]. 中国实验血液学杂志, 2024, 32(4): 1152-1159.
[21] 侯健, 王君颖. 多发性骨髓瘤免疫微环境的研究进展[J]. 肿瘤防治研究, 2022, 49(5): 375-378. doi: 10.3971/j.issn.1000-8578.2022.21.1427
[22] Shi L, Qin X, Wang H, et al. Elevated neutrophil-to-lymphocyte ratio and monocyte-to-lymphocyte ratio and decreased platelet-to-lymphocyte ratio are associated with poor prognosis in multiple myeloma[J]. Oncotarget, 2017, 8(12): 18792-18801. doi: 10.18632/oncotarget.13320
[23] 龚盈盈, 闫晓爽, 王叶敏, 等. 多发性骨髓瘤患者的临床特征及预后因素分析[J]. 中国实验血液学杂志, 2021, 29(3): 772-780.
[24] 罗清文, 陈万紫. 274例多发性骨髓瘤间期荧光原位杂交技术检测结果分析[J]. 检验医学与临床, 2019, 16(7): 947-949. doi: 10.3969/j.issn.1672-9455.2019.07.023
[25] 胡斌, 刘林湘, 陈丹丹. 100例多发性骨髓瘤患者荧光原位杂交结果汇总分析[J]. 河南医学研究, 2017, 26(17): 3075-3077. doi: 10.3969/j.issn.1004-437X.2017.17.002
[26] 刘菲阳, 成倩, 宋奎, 等. 湖南省多发性骨髓瘤诊治现状[J]. 中南大学学报(医学版), 2022, 47(4): 497-504.
[27] Tyczyńska A, Zaucha J. At what point are we on the way to optimally treat multiple myeloma patients over 75 years of age in 2023?[J]. Adv Clin Exp Med, 2024, 33(4): 409-418.
[28] Han F, Sheng N, Sheng C, et al. The diagnostic and prognostic value of haematologic parameters in multiple myeloma patients[J]. Hematology, 2023, 28(1): 2240145. doi: 10.1080/16078454.2023.2240145
[29] 徐一方, 韩海心, 杨讯. 不同化疗方案治疗多发性骨髓瘤的疗效及并发感染的对比研究[J]. 实用癌症杂志, 2023, 38(10): 1658-1660, 1676. doi: 10.3969/j.issn.1001-5930.2023.10.022
-

图(5)
表(5)
计量
- 文章访问数: 596
- PDF下载数: 59
- 施引文献: 0