
A retrospective study of polatuzumab vedotin-based combination regimens in the treatment of newly diagnosed diffuse large B-Cell lymphoma
-
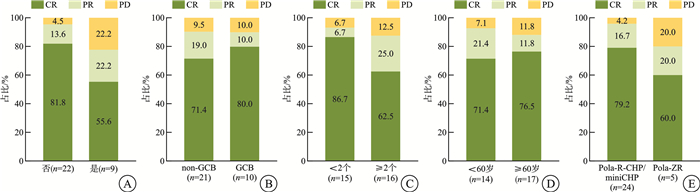
摘要: 目的 探讨基于维泊妥珠单抗(Pola)的联合治疗方案在初治弥漫性大B细胞淋巴瘤(DLBCL)患者中的疗效与安全性。方法 对2023年4月—2025年2月在华中科技大学同济医学院附属协和医院行Pola联合治疗的31例初治DLBCL患者进行回顾性病例资料整理与分析。结果 共纳入31例患者,中位年龄62(18~81)岁,其中非生发中心B细胞(non-GCB)型21例(67.7%),双表达淋巴瘤(DEL)9例(29.0%),结外受累27例(87.1%),国际预后指数评分3~5分者18例(58.1%)。使用Pola-R-CHP(Pola联合利妥昔单抗、环磷酰胺、多柔比星及泼尼松)方案治疗者22例,Pola-miniCHP方案2例,Pola-ZR(Pola联合泽布替尼和利妥昔单抗)方案5例,其余2例分别为Pola-BR(Pola联合苯达莫司汀和利妥昔单抗)及Pola-R-GDP(Pola联合利妥昔单抗、吉西他滨、地塞米松和顺铂)方案。疗效评估显示,客观缓解率(ORR)为90.3%,完全缓解(CR)率为74.2%,疾病进展(PD)率为9.7%。DEL患者的ORR为77.8%,CR率为55.6%;non-GCB患者的ORR为90.5%,CR率为71.4%。老年患者(≥60岁)ORR为92.9%,CR率为71.4%。Pola-R-CHP/miniCHP组ORR为95.8%,CR率为79.2%;Pola-ZR组ORR为80.0%,CR率为60.0%。预期1年总体生存(OS)率为92.4%,无进展生存(PFS)率为84.9%。不同分组在ORR、CR率、OS率和PFS率方面差异无统计学意义。治疗过程中,最常见的血液学相关不良事件包括贫血(轻度58.1%、重度12.9%),中性粒细胞减少(轻度16.1%、重度19.4%)及白细胞减少(轻度25.8%、重度19.4%);非血液系统不良事件包括肺部感染(29.0%)、食欲减退(12.9%)、恶心与呕吐(各9.7%)。结论 在真实世界研究背景下,基于Pola的联合方案在初治DLBCL患者中显示出较高的缓解率与较好耐受性。在DEL、non-GCB、伴结外侵犯及老年等高风险人群中亦表现出潜在的治疗前景,有待进一步研究以明确其临床获益。
-
关键词:
- 弥漫性大B细胞淋巴瘤 /
- 维泊妥珠单抗 /
- 初治 /
- 疗效 /
- 安全性
Abstract: Objective To investigate the efficacy and safety of polatuzumab vedotin(Pola) -based combination regimens in patients with newly diagnosed diffuse large B-cell lymphoma(DLBCL).Methods A retrospective analysis was conducted on the clinical data of 31 patients with newly diagnosed DLBCL who received Pola-based combination regimens at Union Hospital, Tongji Medical College, Huazhong University of Science and Technology from April 2023 to February 2025.Results A total of 31 patients were included, with a median age of 62(range 18-81) years. Among them, 21 patients(67.7%) had the non-germinal center B-cell-like(non-GCB) subtype, 9 patients(29.0%) had double-expressor lymphoma(DEL), and 27 patients(87.1%) presented with extranodal involvement. Eighteen patients(58.1%) had an IPI score of 3-5. The treatment regimens included Pola-R-CHP(n=22), Pola-miniCHP(n=2), Pola-ZR(n=5), Pola-BR(n=1) and Pola-R-GDP(n=1). The objective response rate(ORR) was 90.3%, with a complete response(CR) rate of 74.2% and a progressive disease(PD) rate of 9.7%. DEL patients had an ORR of 77.8% and a CR rate of 55.6%; non-GCB patients had an ORR of 90.5% and a CR rate of 71.4%. Elderly patients(≥60 years) had an ORR of 92.9% and a CR rate of 71.4%. The ORR and CR rate were 95.8% and 79.2% in the Pola-R-CHP/miniCHP group, and 80.0% and 60.0% in the Pola-ZR group, respectively. The estimated 1-year overall survival(OS) and progression-free survival(PFS) rates were 92.4% and 84.9%, respectively. There were no statistically significant differences in ORR, CR, OS or PFS among the subgroups. The most common treatment-related adverse events were anemia(grade 1-2: 58.1%, grade 3-4: 12.9%), neutropenia(grade 1-2: 16.1%, grade 3-4: 19.4%), and leukopenia(grade 1-2: 25.8%, grade 3-4: 19.4%); the most frequent non-hematological toxicities included pulmonary infection(29.0%), decreased appetite(12.9%), nausea and vomiting(each 9.7%).Conclusion In real-world settings, Pola-based combination regimens demonstrated favorable remission rates and manageable safety profiles in newly diagnosed DLBCL patients, with potential clinical value in high-risk subgroups such as DEL, non-GCB subtype, extranodal involvement, and elderly patients. Further investigation is warranted to confirm these benefits.-
Key words:
- diffuse large B-cell lymphoma /
- polatuzumab vedotin /
- newly diagnosed /
- efficacy /
- safety
-

-
表 1 31例初治DLBCL患者基本情况
中位数(范围),例(%) 特征 数值 中位年龄/岁 62(18~81) 性别 男 13(41.9) 女 18(58.1) ECOG评分/分 0~1 19(61.3) ≥ 2 12(38.7) B症状 无 20(64.5) 有 11(35.5) 诊断时乳酸脱氢酶 正常 11(35.5) 升高 20(64.5) Lugano分期/期 Ⅰ~Ⅱ 7(22.6) Ⅲ~Ⅳ 24(77.4) IPI评分/分 0~2 13(41.9) 3~5 18(58.1) 细胞起源 GCB 10(32.3) non-GCB 21(67.7) DEL 否 22(71.0) 是 9(29.0) 骨髓受累 无 30(96.8) 有 1(3.2) 结外累及 无 4(12.9) 有 27(87.1) 结外病灶数(限结外受累患者)/个 <2 11(40.7) ≥ 2 16(59.3) 中位随访时间/d 180(42~657) 中位PFS时间/d 158(42~625) 注:以下3种情况中出现任何1种即有B症状:①不明原因发热>38℃,连续3 d以上,排除感染的原因;②夜间盗汗(可浸透衣物);③体重于诊断前半年内下降>10%。  下载: 导出CSV
下载: 导出CSV
表 2 患者治疗相关不良反应情况
例(%) 不良反应类别 1~2级 3~4级 血液学不良反应 贫血 18(58.1) 4(12.9) 血小板减少 3(9.7) 5(16.1) 白细胞减少 8(25.8) 6(19.4) 中性粒细胞减少 5(16.1) 6(19.4) 发热性中性粒细胞减少 4(12.9) 非血液学不良反应 肺部感染 9(29.0) 过敏 1(3.2) 心律失常 2(6.5) 肝功能不良 2(6.5) 食欲减退 4(12.9) 恶心 3(9.7) 呕吐 3(9.7)
下载: 导出CSV
-
[1] Geng H, Jia S, Zhang Y, et al. Efficacy and safety of zanubrutinib plus R-CHOP in treatment of non-GCB DLBCL with extranodal involvement[J]. Front Immunol, 2023, 14: 1219167. doi: 10.3389/fimmu.2023.1219167
[2] Sehn LH, Salles G. Diffuse Large B-Cell Lymphoma[J]. N Engl J Med, 2021, 384(9): 842-858. doi: 10.1056/NEJMra2027612
[3] Poletto S, Novo M, Paruzzo L, et al. Treatment strategies for patients with diffuse large B-cell lymphoma[J]. Cancer Treat Rev, 2022, 110: 102443. doi: 10.1016/j.ctrv.2022.102443
[4] 张钰奇, 武盈盈, 张奥, 等. 基于奥布替尼的联合方案治疗28例初治弥漫性大B细胞淋巴瘤的疗效与安全性分析[J]. 临床血液学杂志, 2024, 37(9): 631-636. doi: 10.13201/j.issn.1004-2806.2024.09.007
[5] McMillan AK, Phillips EH, Kirkwood AA, et al. Favourable outcomes for high-risk diffuse large B-cell lymphoma(IPI 3-5) treated with front-line R-CODOX-M/R-IVAC chemotherapy: results of a phase 2 UK NCRI trial[J]. Ann Oncol, 2020, 31(9): 1251-1259. doi: 10.1016/j.annonc.2020.05.016
[6] Zelenetz AD, Gordon LI, Abramson JS, et al. NCCN Guidelines® Insights: B-Cell Lymphomas, Version 6.2023[J]. J Natl Compr Canc Netw, 2023, 21(11): 1118-1131. doi: 10.6004/jnccn.2023.0057
[7] 中国临床肿瘤学会指南工作委员会. 中国临床肿瘤学会(CSCO)淋巴瘤诊疗指南2023[M]. 北京: 人民卫生出版社, 2023: 28.
[8] Tilly H, Morschhauser F, Sehn LH, et al. Polatuzumab vedotin in previously untreated diffuse large B-cell lymphoma[J]. N Engl J Med, 2022, 386(4): 351-363. doi: 10.1056/NEJMoa2115304
[9] Deng R, Gibiansky L, Lu T, et al. Population pharmacokinetics and exposure-response analyses of polatuzumab vedotin in patients with previously untreated DLBCL from the POLARIX study[J]. CPT Pharmacometrics Syst Pharmacol, 2024, 13(6): 1055-1066. doi: 10.1002/psp4.13141
[10] Cheson BD, Fisher RI, Barrington SF, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification[J]. J Clin Oncol, 2014, 32(27): 3059-3068. doi: 10.1200/JCO.2013.54.8800
[11] Freites-Martinez A, Santana N, Arias-Santiago S, et al. Using the common terminology criteria for adverse events(CTCAE-Version 5.0) to evaluate the severity of adverse events of anticancer therapies[J]. Actas Dermosifiliogr(Engl Ed), 2021, 112(1): 90-92. doi: 10.1016/j.ad.2019.05.009
[12] Shanthi D, Vinotha S. A comprehensive review of Polatuzumab vedotin: Mechanisms, clinical applications, and future prospects[J]. Natl Board Exam J Med Sci, 2024, 2(3): 256-263.
[13] Dornan D, Bennett F, Chen Y, et al. Therapeutic potential of an anti-CD79b antibody-drug conjugate, anti-CD79b-vc-MMAE, for the treatment of non-Hodgkin lymphoma[J]. Blood, 2009, 114(13): 2721-2729. doi: 10.1182/blood-2009-02-205500
[14] Song Y, Tilly H, Rai S, et al. Polatuzumab vedotin in previously untreated DLBCL: an Asia subpopulation analysis from the phase 3 POLARIX trial[J]. Blood, 2023, 141(16): 1971-1981. doi: 10.1182/blood.2022017734
[15] Mehta A, Verma A, Gupta G, et al. Double hit and double expresser diffuse large B cell lymphoma subtypes: discrete subtypes and major predictors of overall survival[J]. Indian J Hematol Blood Transfus, 2020, 36(4): 627-634. doi: 10.1007/s12288-019-01248-w
[16] Zhao P, Zhao S, Huang C, et al. Efficacy and safety of Polatuzumab vedotin plus rituximab, cyclophosphamide, doxorubicin and prednisone for previously untreated diffuse large B-cell lymphoma: a real-world, multi-center, retrospective cohort study[J]. Hematol Oncol, 2025, 43(1): e70017. doi: 10.1002/hon.70017
[17] Russler-Germain DA, Cliff ERS, Bartlett NL. Cell-of-origin effect of polatuzumab vedotin in diffuse large B-cell lymphoma: no ordinary subgroup analysis[J]. Blood, 2023, 142(25): 2216-2219. doi: 10.1182/blood.2023022048
[18] Gupta V, Singh V, Bajwa R, et al. Site-specific survival of extra nodal diffuse large B-cell lymphoma and comparison with gastrointestinal diffuse large B-cell lymphoma[J]. J Hematol, 2022, 11(2): 45-54. doi: 10.14740/jh984
[19] Ayers EC, Smith SM. Diffuse large B-cell lymphoma in the older and frail patient[J]. Cancers(Basel), 2025, 17(5): 885.
[20] Jardin F, Tilly H. Chemotherapy-free treatment in unfit patients aged 75 years and older with DLBCL: toward a new paradigm?[J]. Lancet Healthy Longev, 2022, 3(7): e453-e454. doi: 10.1016/S2666-7568(22)00150-7
-
计量
- 文章访问数: 70
- 施引文献: 0