
A single-center, real-world study of efficacy and safety of first-line venetoclax-based regimens in treating newly diagnosed acute myeloid leukemia
-
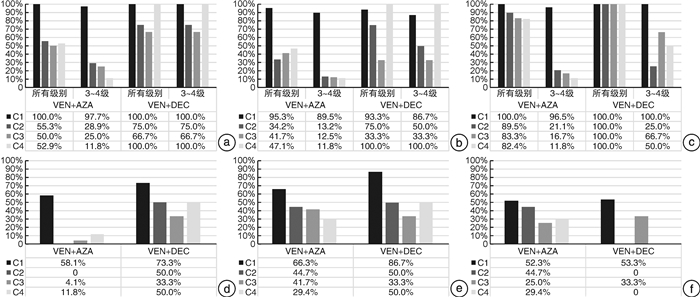
摘要: 目的 靶向药物BCL-2抑制剂维奈克拉(venetoclax,VEN)的出现革新了急性髓系白血病(acute myeloid leukemia,AML)的治疗格局,尤其是对于老年或不适合强化疗的患者,其与去甲基化药物(hypomethylating agents,HMAs)的联合方案在临床中得以广泛应用。我们对本中心近4年余VEN联合方案一线治疗在新诊断AML患者的真实世界应用情况进行回顾性研究,以期为临床实践提供参考。方法 回顾性收集和分析2019年8月至2024年2月首次接受VEN联合方案一线治疗的110例新诊断AML患者的临床资料,后续治疗策略由临床医生根据患者综合情况进行动态调整。结果 中位随访时间14.8(0.2~37.1)个月,中位VEN一线联合方案疗程数1(1~8)个,中位总抗AML治疗(非临床试验)疗程数3(1~10)个。应用人群:VEN一线联合方案已广泛应用于患者相关特征和AML疾病相关特征各异的新诊断AML患者,应用人群多伴有基础合并症(74.5%),且绝大多数在启动VEN联合治疗前存在≥3级血常规异常(98.2%)。应用方案:诱导治疗以VEN+阿扎胞苷(azacitidine,AZA)为主(78.2%),29.1%的患者在仅接受诱导治疗后即失访或死亡,诱导治疗后继续治疗的患者中44.9%进行治疗策略调整,仅23.6%的患者持续接受≥4个疗程VEN+HMAs±FLT3抑制剂治疗。治疗反应:VEN一线联合方案诱导治疗的复合完全缓解率(composite complete response,cCR)为80.2%,微小残留病(minimal residual disease,MRD)转阴率为69.2%;总队列中达到cCR或MRD转阴患者的中位总生存期(overall survival,OS)和中位无事件生存期(event-free survival,EFS)均显著优于未达到者[达到cCR组vs未达到cCR组中位OS:37.1 vs 3.5个月(P<0.001),中位EFS:14.8 vs 0.9个月(P<0.001);达到MRD-组与未达到MRD-组中位OS:37.1 vs 3.5个月(P<0.001),中位EFS:14.8 vs 1.3个月(P<0.001)];总队列复发率为30.8%。安全性:总体耐受性较好,VEN+HMAs持续治疗的血液学毒性以第1个疗程为著,第2~4个疗程VEN+AZA组的3~4级血液学毒性和感染发生率总体低于VEN+地西他滨组,且VEN+AZA组随疗程增加呈下降趋势。结论 VEN联合方案一线治疗新诊断AML患者能够较快获得高治疗反应率,不良反应总体可耐受,且以第1个疗程为著。真实世界中VEN一线联合方案诱导后进行治疗策略调整情况常见,获得缓解或MRD转阴的患者生存获益显著。仍有相当比例的患者未能从VEN一线联合方案中获益或复发,亟待寻求优化解决方案。Abstract: Objective The advent of targeted drug BCL-2 inhibitor venetoclax(VEN) has revolutionized the treatment pattern of acute myeloid leukemia(AML), especially for elderly patients or those ineligible for intensive chemotherapy. Its combination regimens with hypomethylating agents(HMAs) have been widely used in clinical practice. We conducted a single-center, retrospective study on the real-world application of VEN-based first-line treatment in newly diagnosed AML patients over the past four years in aim of providing reference for clinical practice.Methods The clinical data of 110 newly diagnosed AML patients who received VEN first-line combination treatment for the first time from August 2019 to February 2024 were retrospectively analyzed.Results The median follow-up time was 14.8(0.2-37.1) months, with a median of 1(1-8) courses of first-line VEN combination therapy and a median of 3(1-10) courses of total treatment courses applied(clinical trials excluded). Application population: The VEN first-line combination therapy has been widely used in newly diagnosed AML patients with different patient-related and AML disease-related characteristics. The application population was often accompanied by underlying comorbidities(74.5%), and the vast majority had ≥ grade 3 blood routine tests abnormalities(98.2%) before initiating VEN combination therapy. Treatment regimens: VEN+azacitidine(AZA) was the main choice of induction therapy(78.2%). 29.1% of patients were lost to follow-up or died after only receiving induction therapy. Among patients who continued treatment after induction therapy, 44.9% underwent treatment strategy adjustments, and only 23.6% continued to receive ≥ 4 courses of VEN+HMAs±FLT3 inhibitor treatment. Treatment response: The composite complete response rate(cCR) induced by VEN first-line combination therapy was 80.2%, and the rate of achieving negative minimal residual disease(MRD) was 69.2%. The median overall survival(OS) and median event-free survival(EFS) of patients who achieved cCR or MRD negative in the overall cohort were significantly better than those without cCR or MRD negative(the median OS of cCR vs non-cCR: 37.1 vs 3.5 months[P<0.001], the median EFS of cCR vs non-cCR: 14.8 vs 0.9 months[P<0.001]; the median OS of MRD- vs non-MRD-: 37.1 vs 3.5 months[P<0.001], the median EFS of MRD- vs non-MRD-: 14.8 vs 1.3 months[P<0.001]). The overall recurrence rate was 30.8%. Safety: Overall toxicities were tolerable, and hematological toxicities of continuous treatment with VEN+HMAs were mainly observed in the first course. The incidence of grade 3-4 hematological toxicities and infection in the VEN+AZA group was generally lower than that in the VEN+decitabine group, and the VEN+AZA group showed a decreasing trend with the increase of treatment courses.Conclusion VEN first-line combination therapy can achieve quick and high response in newly diagnosed AML patients, overall adverse events are tolerable, with the first course being the most notable. In real-world settings, it is common to adjust treatment strategies after first-line VEN induction therapy, patients who achieve remission or MRD negative can benefit from significant survival advantage. However, there is still a considerable proportion of patients who could not benefit from VEN-based first-line therapy or experienced relapse, optimized solutions are urgently needed.
-
Key words:
- venetoclax /
- acute myeloid leukemia /
- real-world study
-

-
表 1 110例新诊断AML患者基线临床特征
例(%) 临床特征 总队列 年龄 <60岁 47(42.7) ≥60岁 63(57.3) 性别 男 58(52.7) 女 52(47.3) 疾病类型 原发性 103(93.6) 继发性 7(6.4) ECOG PS评分 0~1分 55(50.0) 2~4分 55(50.0) 伴基础合并症 是 82(74.5) 心脑血管疾病 38(34.5) 内分泌代谢疾病 26(23.6) 呼吸系统疾病 14(12.7) 否 28(25.5) ELN危险度分层 低危 26(23.6) 中危 34(30.9) 高危 33(30.0) 结果缺失 17(15.5) 分子生物学特征 FLT3-ITD/TKD 30(27.3) IDH1/2 23(20.9) DNMT3A 20(18.2) NPM1 19(17.3) TET2 11(10.0) TP53 10(9.1) RUNX1 9(8.2) K/N-RAS 9(8.2) ASXL1 8(7.3) CEBPA 8(7.3) BCOR 7(6.4) 结果缺失 14(12.7) ≥3级血常规异常 108(98.2) 贫血 88(80.0) 血小板减少 67(60.9) 中性粒细胞减少 63(57.3)  下载: 导出CSV
下载: 导出CSV
表 2 91例可评价疗效的新诊断AML患者治疗反应率
例(%) 组别 总例数 第1个疗程疗效 最佳疗效 ORR cCR cCRMRD- ORR cCR cCRMRD- 年龄 <60岁 44 42(95.5) 36(81.8) 32(88.9) 43(97.7) 42(95.5) 41(97.6) ≥60岁 47 42(89.4) 37(78.7) 31(83.8) 45(95.7) 42(89.4) 40(95.2) 危险度分层 低危 21 21(100.0) 15(71.4) 13(86.7) 21(100.0) 20(95.2) 19(95.0) 中危 31 27(87.1) 25(80.6) 20(80.0) 30(96.8) 28(90.3) 26(92.9) 高危 28 25(89.3) 23(82.1) 20(87.0) 26(92.9) 25(89.3) 25(100.0) 分子学特征 FLT3突变 是 28 26(92.9) 22(78.6) 19(86.4) 27(96.4) 25(89.3) 25(100.0) 否 55 50(90.9) 44(80.0) 37(84.1) 52(94.5) 51(92.7) 48(94.1) IDH1/2突变 是 20 20(100.0) 18(90.0) 17(94.4) 20(100.0) 19(95.0) 19(100.0) 否 63 56(88.9) 48(76.2) 38(79.2) 60(95.2) 57(90.5) 54(94.7) NPM1突变 是 17 17(100.0) 15(88.2) 14(93.3) 17(100.0) 16(94.1) 16(100.0) 否 66 59(89.4) 51(77.3) 41(80.4) 63(95.5) 60(90.9) 57(95.0) TP53突变 是 10 7(70.0) 6(60.0) 6(100.0) 8(80.0) 7(70.0) 7(100.0) 否 73 69(94.5) 60(82.2) 49(81.7) 72(98.6) 69(94.5) 66(95.7)
下载: 导出CSV
-
[1] DiNardo CD, Jonas BA, Pullarkat V, et al. Azacitidine and Venetoclax in Previously Untreated Acute Myeloid Leukemia[J]. N Engl J Med, 2020, 383(7): 617-629. doi: 10.1056/NEJMoa2012971
[2] 中国临床肿瘤学会白血病专家委员会. 维奈克拉治疗恶性血液病临床应用指导原则(2021年版)[J]. 白血病·淋巴瘤, 2021, 30(12): 710-718. doi: 10.3760/cma.j.cn115356-20210811-00175
[3] Khoury JD, Solary E, Abla O, et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms[J]. Leukemia, 2022, 36(7): 1703-1719. doi: 10.1038/s41375-022-01613-1
[4] Döhner H, Wei AH, Appelbaum FR, et al. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN[J]. Blood, 2022, 140(12): 1345-1377. doi: 10.1182/blood.2022016867
[5] Freites-Martinez A, Santana N, Arias-Santiago S, et al. Using the Common Terminology Criteria for Adverse Events(CTCAE-Version 5.0) to Evaluate the Severity of Adverse Events of Anticancer Therapies[J]. Actas Dermosifiliogr(Engl Ed), 2021, 112(1): 90-92. doi: 10.1016/j.ad.2019.05.009
[6] 余国攀, 尹昭, 蒋玲, 等. 真实世界中维奈克拉联合方案一线治疗新诊断unfit-AML的疗效和影响因素[J]. 兰州大学学报(医学版), 2022, 48(12): 34-40, 46. https://www.cnki.com.cn/Article/CJFDTOTAL-LZYX202212007.htm
[7] 于文静, 贾晋松, 王婧, 等. 维奈克拉联合阿扎胞苷治疗急性髓系白血病的近期疗效: 单中心数据[J]. 中华血液学杂志, 2022, 43(2): 134-140. https://www.cnki.com.cn/Article/CJFDTOTAL-YYPF202403004.htm
[8] 孙立, 叶少杰, 周楠, 等. 维奈克拉联合阿扎胞苷治疗不适合标准化疗的新诊断急性髓系白血病疗效分析: 单中心数据[J]. 中华血液学杂志, 2022, 43(10): 826-832. doi: 10.3760/cma.j.issn.0253-2727.2022.10.005
[9] Oyogoa E, Traer E, Tyner J, et al. Building on Foundations: Venetoclax-Based Combinations in the Treatment of Acute Myeloid Leukemia[J]. Cancers(Basel), 2023, 15(14): 3589.
[10] Short NJ, Kantarjian H. Choosing between intensive and less intensive front-line treatment approaches for older patients with newly diagnosed acute myeloid leukaemia[J]. Lancet Haematol, 2022, 9(7): e535-e545. doi: 10.1016/S2352-3026(22)00167-3
[11] Pratz KW, Jonas BA, Pullarkat V, et al. Long-term follow-up of VIALE-A: Venetoclax and azacitidine in chemotherapy-ineligible untreated acute myeloid leukemia[J]. Am J Hematol, 2024, Epub ahead of print. DOI:
10.1002/ajh.27246 .[12] Hu M, Li W, Zhang Y, et al. Venetoclax in adult acute myeloid leukemia[J]. Biomed Pharmacother, 2023, 168: 115820. doi: 10.1016/j.biopha.2023.115820
[13] Patel KK, Zeidan AM, Shallis RM, et al. Cost-effectiveness of azacitidine and venetoclax in unfit patients with previously untreated acute myeloid leukemia[J]. Blood Adv, 2021, 5(4): 994-1002. doi: 10.1182/bloodadvances.2020003902
[14] 赵馨然, 莫璇, 赵瑾, 等. 维奈克拉治疗不适合强诱导化疗的新诊断急性髓系白血病: 真实世界使用以及医疗资源利用情况[J]. 中国药物经济学, 2023, 18(5): 29-36. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYWA202305005.htm
[15] Gangat N, Ilyas R, Johnson IM, et al. Outcome of patients with acute myeloid leukemia following failure of frontline venetoclax plus hypomethylating agent therapy[J]. Haematologica, 2023, 108(11): 3170-3174. doi: 10.3324/haematol.2022.282677
[16] Qin Y, Kuang P, Liu T. Venetoclax combined with hypomethylating agents or low-dose cytarabine as induction chemotherapy for patients with untreated acute myeloid leukemia ineligible for intensive chemotherapy: a systematic review and meta-analysis[J]. Clin Exp Med, 2023, 23(2): 219-227.
[17] Apel A, Moshe Y, Ofran Y, et al. Venetoclax combinations induce high response rates in newly diagnosed acute myeloid leukemia patients ineligible for intensive chemotherapy in routine practice[J]. Am J Hematol, 2021, 96(7): 790-795. doi: 10.1002/ajh.26190
[18] Gangat N, Johnson I, McCullough K, et al. Molecular predictors of response to venetoclax plus hypomethylating agent in treatment-naive acute myeloid leukemia[J]. Haematologica, 2022, 107(10): 2501-2505. doi: 10.3324/haematol.2022.281214
[19] Gangat N, Karrar O, Iftikhar M, et al. Venetoclax and hypomethylating agent combination therapy in newly diagnosed acute myeloid leukemia: Genotype signatures for response and survival among 301 consecutive patients[J]. Am J Hematol, 2024, 99(2): 193-202. doi: 10.1002/ajh.27138
[20] Bataller A, Bazinet A, DiNardo CD, et al. Prognostic risk signature in patients with acute myeloid leukemia treated with hypomethylating agents and venetoclax[J]. Blood Adv, 2024, 8(4): 927-935. doi: 10.1182/bloodadvances.2023011757
[21] Kayser S, Levis MJ. The clinical impact of the molecular landscape of acute myeloid leukemia[J]. Haematologica, 2023, 108(2): 308-320. doi: 10.3324/haematol.2022.280801
[22] Badar T, Nanaa A, Atallah E, et al. Comparing venetoclax in combination with hypomethylating agents to hypomethylating agent-based therapies for treatment naive TP53-mutated acute myeloid leukemia: results from the Consortium on Myeloid Malignancies and Neoplastic Diseases(COMMAND)[J]. Blood Cancer J, 2024, 14(1): 32. doi: 10.1038/s41408-024-01000-2
[23] Craddock C, Versluis J, Labopin M, et al. Distinct factors determine the kinetics of disease relapse in adults transplanted for acute myeloid leukaemia[J]. J Internal Med, 2018, 283(4): 371-379. doi: 10.1111/joim.12720
[24] 姜尔烈, 郑亚伟. 靶向治疗及免疫治疗时代造血干细胞移植在急性白血病中的应用[J]. 临床血液学杂志, 2023, 36(9): 615-621. doi: 10.13201/j.issn.1004-2806.2023.09.002
[25] Kennedy VE, Hui G, Azenkot T, et al. Outcomes of allogeneic transplantation after hypomethylating agents with venetoclax in acute myeloid leukemia[J]. Am J Hematol, 2022, 97(6): E191-E194.
[26] Pollyea DA, Pratz K, Letai A, et al. Venetoclax with azacitidine or decitabine in patients with newly diagnosed acute myeloid leukemia: Long term follow-up from a phase 1b study[J]. Am J Hematol, 2021, 96(2): 208-217. doi: 10.1002/ajh.26039
[27] Zhu LX, Chen RR, Wang LL, et al. A real-world study of infectious complications of venetoclax combined with decitabine or azacitidine in adult acute myeloid leukemia[J]. Support Care Cancer, 2022, 30(8): 7031-7038.
[28] Candoni A, Lazzarotto D, Papayannidis C, et al. Prospective multicenter study on infectious complications and clinical outcome of 230 unfit acute myeloid leukemia patients receiving first-line therapy with hypomethylating agents alone or in combination with Venetoclax[J]. Am J Hematol, 2023, 98(4): E80-E83.
-
计量
- 文章访问数: 330
- 施引文献: 0