
Clinical efficacy and safety of CLAG+Ven as salvage therapy for relapsed/refractory acute myeloid leukemia: A single-center, single-arm clinical study
-
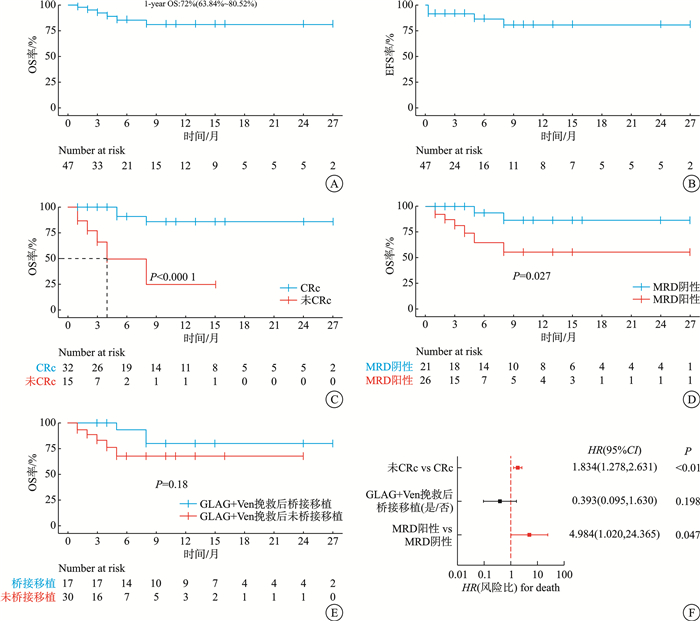
摘要: 目的 研究维奈克拉(Ven)联合CLAG方案挽救性治疗复发难治急性髓系白血病(RR-AML)的疗效和安全性。方法 开展单中心单臂临床研究使用CLAG+Ven挽救治疗RR-AML,主要终点为复合缓解(CRc)率,次要终点为总反应率(ORR)、可检测残留病(MRD)、无事件生存(EFS)、总生存(OS)和安全性分析。结果 2021年7月—2024年12月共有47例RR-AML患者接受1个疗程CLAG+Ven治疗并完成疗效和安全性评估,中位年龄42(18~65)岁,37例(78.7%)患者获得治疗反应,其中32例(68.1%)达到CRc,21例(65.6%)获得MRD阴性CRc。欧洲白血病网络低、中、高危组或细胞遗传学非高危和高危组患者的CRc率均差异无统计学意义。亚组分析显示既往去甲基化药物(HMA)暴露对患者获得CRc不利。中位随访13.0(8.7~17.3)个月,中位OS、中位EFS均未达到,1年OS率为72%(95%CI:63.84%~80.52%)。CLAG+Ven治疗患者中性粒细胞恢复至>1×109/L的中位时间为18(7~58) d,30 d和60 d死亡率分别为2.1%和6.4%。结论 CLAG+Ven方案挽救治疗RR-AML有较好疗效,耐受性良好。Abstract: Objective To investigate the clinical efficacy and safety of the CLAG(Cladribine, Cytarabine, and G-CSF) plus Venetoclax(Ven) regimen as salvage therapy for relapsed/refractory acute myeloid leukemia(RR-AML).Methods A single-center, single-arm study was performed to evaluate the clinical efficacy and safety of CLAG+Ven regimen in patients with RR-AML. The primary endpoint was the composite complete remission(CRc) rate. Secondary endpoints included the overall response rate(ORR), measurable residual disease(MRD), event-free survival(EFS), overall survival(OS), and safety analysis.Results From July 2021 to December 2024, a total of 47 patients with RR-AML were included, who have received one course of CLAG+Ven therapy and completed response evaluation, with a median age of 42(range 18-65) years. Thirty-seven patients(78.7%) acquired response, including 32(68.1%) with CRc and 21(65.6%) with MRD-negative CRc. There were no statistical differences in the CRc rates among the different risk groups based on ELN stratification and cytogenetic classification. Subgroup analysis showed that prior exposure to hypomethylating agents(HMAs) was associated with a poor CRc. With a median follow-up of 13(8.7-17.3) months, median OS and EFS were not reached, and the 1-year OS rate was 72%(95%CI: 63.84%-80.52%). The median time for neutrophil recovery(Neu>1×109/L) was 18(range 7-58) days, with the 30-and 60-day mortality rates of 2.1% and 6.4%, respectively.Conclusion The CLAG+Ven regimen as salvage therapy demonstrated a promising efficacy in patients with RR-AML and was well-tolerated.
-
Key words:
- Venetoclax /
- CLAG /
- refractory/relapsed /
- salvage therapy /
- acute myeloid leukemia
-

-
表 1 患者临床基线特征
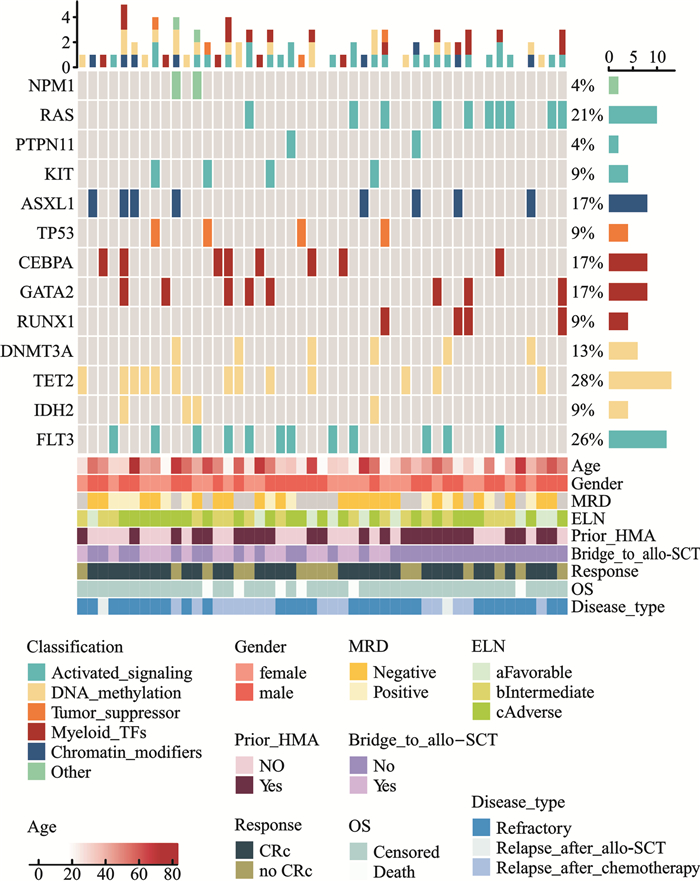
中位数(范围),例(%) 特征 数值 男/女 25 /22 年龄/岁 42(18~65) AML类型 原发 45(95.7) 继发 2(4.3) 疾病类型 原发难治 29(61.7) 化疗或移植后复发 18(38.3) 既往HMA暴露 24(51.1) Ven减量调整 16(34.0) 既往移植 2(4.3) 既往化疗中位周期/疗程 2(1~12) ELN分层 低危 9(19.1) 中危 16(34.0) 高危 22(46.8) 细胞遗传学分型 非高危 31(66.0) 高危 15(31.9) 缺失 1(2.1) 联合FLT3抑制剂 12(25.5) 桥接移植 17(36.2) 基因突变 TET2 13(28) FLT3 12(26) RAS 10(21) ASXL1 8(17) CEBPA 8(17) GATA2 8(17) DNMT3A 6(13) TP53 4(9) KIT 4(9) IDH2 4(9) NPM1 2(4) PTPN11 2(4)  下载: 导出CSV
下载: 导出CSV
表 2 治疗反应
例(%),中位数(范围) 指标 数值 ORR 37(78.7) CRc 32(68.1) CR 16(34.0) CRi 16(34.0) PR 5(10.6) NR 10(21.2) MRD-CRc(n=32) 21(65.6) 随访时间/月 13(8.7~17.3) 复发(n=32) 7(21.9) 死亡 9(19.1)
下载: 导出CSV
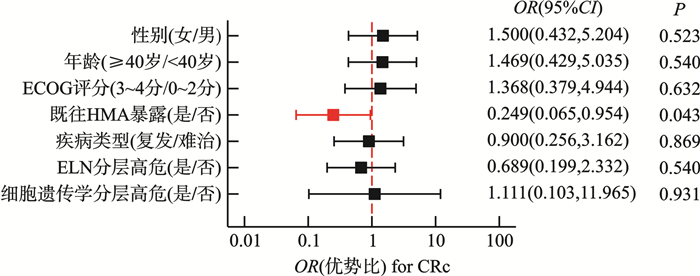
表 3 单因素logistic回归分析CRc影响因素
变量 OR 95%CI P 性别/(女vs男) 1.500 0.432~5.204 0.523 年龄/(≥40岁vs < 40岁) 1.469 0.429~5.035 0.540 ECOG评分/(3~4分vs 0~2分) 1.368 0.379~4.944 0.632 白细胞计数/(≥20×109/L vs < 20×109/L) 0.989 0.264~3.700 0.987 既往HMA暴露/(是vs否) 0.249 0.065~0.954 0.043 Ven减量调整/(是vs否) 1.467 0.410~5.249 0.556 疾病类型/(复发vs原发耐药) 0.900 0.256~3.162 0.869 ELN危险分层/(高危vs非高危) 0.681 0.199~2.332 0.540 细胞遗传学/(高危vs非高危) 1.111 0.103~11.965 0.931 基因突变 RAS/(是vs否) 0.635 0.149~2.701 0.538 KIT/(是vs否) 1.448 0.138~15.206 0.758 ASXL1/(是vs否) 1.500 0.265~8.489 0.647 TP53/(是vs否) 0.433 0.055~3.418 0.427 CEBPA/(是vs否) 1.500 0.265~8.489 0.647 GATA2/(是vs否) 0.741 0.152~3.613 0.711 RUNX1/(是vs否) 0.433 0.055~3.418 0.427 DNMT3A/(是vs否) 0.414 0.073~2.348 0.319 TET2/(是vs否) 0.667 0.175~2.543 0.553 FLT3/(是vs否) 1.565 0.356~6.885 0.553
下载: 导出CSV
表 4 治疗相关不良反应
例(%) 不良反应 所有分级 分级≥3级 中性粒细胞减少 47(100.0) 47(100.0) 血小板减少 47(100.0) 47(100.0) 贫血 47(100.0) 46(97.9) 中性粒细胞减少伴发热 30(63.8) 24(51.1) 肺炎 17(36.2) 13(27.7) 败血症 7(14.9) 7(14.9) 恶心呕吐 15(31.9) 5(10.6) 腹泻 6(12.8) 0 出血(阴道、胃肠道、肺部) 4(8.5) 1(2.1) 过敏反应 5(10.6) 0 心衰 3(6.4) 0 肿瘤溶解综合征 3(6.4) 1(2.1) 肝肾功能不全 4(8.5) 2(4.3)
下载: 导出CSV
-
[1] Mohamed Jiffry MZ, Kloss R, Ahmed-Khan M, et al. A review of treatment options employed in relapsed/refractory AML[J]. Hematology, 2023, 28(1): 2196482. doi: 10.1080/16078454.2023.2196482
[2] National Comprehensive Cancer Network. Acute Myeloid Leukemia(version 2)[EB/OL]. [2024-12-15].
https://www.nccn.org/professionals/physician_gls/pdf/aml.pdf (2024).[3] 中华医学会血液学分会白血病淋巴瘤学组. 中国复发难治性急性髓系白血病诊疗指南(2023年版)[J]. 中华血液学杂志, 2023, 44(9): 713-716.
[4] Wierzbowska A, Robak T, Pluta A, et al. Cladribine combined with high doses of Arabinoside cytosine, mitoxantrone, and G-CSF(CLAG-M)is a highly effective salvage regimen in patients with refractory and relapsed acute myeloid leukemia of the poor risk: a final report of the Polish Adult Leukemia Group[J]. Eur J Haematol, 2008, 80(2): 115-126. doi: 10.1111/j.1600-0609.2007.00988.x
[5] Patzke CL, Duffy AP, Duong VH, et al. Comparison of high-dose cytarabine, mitoxantrone, and pegaspargase(HAM-pegA)to high-dose cytarabine, mitoxantrone, cladribine, and filgrastim(CLAG-M)as first-line salvage cytotoxic chemotherapy for relapsed/refractory acute myeloid leukemia[J]. J Clin Med, 2020, 9(2): 536. doi: 10.3390/jcm9020536
[6] Mushtaq MU, Harrington AM, Chaudhary SG, et al. Comparison of salvage chemotherapy regimens and prognostic significance of minimal residual disease in relapsed/refractory acute myeloid leukemia[J]. Leuk Lymphoma, 2021, 62(1): 158-166. doi: 10.1080/10428194.2020.1821009
[7] Kadia TM, Reville PK, Borthakur G, et al. Venetoclax plus intensive chemotherapy with cladribine, idarubicin, and cytarabine in patients with newly diagnosed acute myeloid leukaemia or high-risk myelodysplastic syndrome: a cohort from a single-centre, single-arm, phase 2 trial[J]. Lancet Haematol, 2021, 8(8): e552-e561. doi: 10.1016/S2352-3026(21)00192-7
[8] DiNardo CD, Lachowiez CA, Takahashi K, et al. Venetoclax combined with FLAG-IDA induction and consolidation in newly diagnosed and relapsed or refractory acute myeloid leukemia[J]. J Clin Oncol, 2021, 39(25): 2768-2778. doi: 10.1200/JCO.20.03736
[9] Lee B, Blackmon A, Ngo D, et al. AML-491 real world practice of FLAG-idarubicin-venetoclax in relapsed refractory AML: a single center experience[J]. Clin Lymphoma Myeloma Leuk, 2022, 22: S256-S257.
[10] Döhner H, Wei AH, Appelbaum FR, et al. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN[J]. Blood, 2022, 140(12): 1345-1377. doi: 10.1182/blood.2022016867
[11] Jin H, Zhang Y, Yu SJ, et al. Venetoclax combined with azacitidine and homoharringtonine in relapsed/refractory AML: a multicenter, phase 2 trial[J]. J Hematol Oncol, 2023, 16(1): 42. doi: 10.1186/s13045-023-01437-1
[12] Yu GP, Zhang Y, Yu SJ, et al. Homoharringtonine added to venetoclax and azacitidine improves outcome and mitigates genetic impact in relapsed/refractory AML: a multicenter cohort study[J]. Clin Cancer Res, 2025, 31(1): 87-97. doi: 10.1158/1078-0432.CCR-24-1332
[13] Yu SJ, Zhang Y, Yu GP, et al. Sorafenib plus triplet therapy with venetoclax, azacitidine and homoharringtonine for refractory/relapsed acute myeloid leukemia with FLT3-ITD: a multicenter phase 2 study[J]. J Intern Med, 2024, 295(2): 216-228. doi: 10.1111/joim.13738
[14] Yao H, Zhang C, Tan X, et al. Efficacy and toxicity of CLAG combined with pegylated liposomal doxorubicin in the treatment of refractory or relapsed acute myeloid leukemia[J]. Cancer Med, 2023, 12(11): 12377-12387. doi: 10.1002/cam4.5938
[15] Raychaudhuri S, Gooley T, Gill Z, et al. Phase Ⅰ trial combining venetoclax with G-CSF, cladribine, cytarabine, and mitoxantrone(CLAG-M)for patients with high-grade myeloid neoplasms[J]. Blood, 2023, 142: 2897. doi: 10.1182/blood-2023-181582
[16] Stomper J, Rotondo JC, Greve G, et al. Hypomethylating agents(HMA)for the treatment of acute myeloid leukemia and myelodysplastic syndromes: mechanisms of resistance and novel HMA-based therapies[J]. Leukemia, 2021, 35(7): 1873-1889. doi: 10.1038/s41375-021-01218-0
[17] Short NJ, Venugopal S, Qiao W, et al. Impact of frontline treatment approach on outcomes in patients with secondary AML with prior hypomethylating agent exposure[J]. J Hematol Oncol, 2022, 15(1): 12. doi: 10.1186/s13045-022-01229-z
[18] Lancet JE, Uy GL, Cortes JE, et al. CPX-351(cytarabine and daunorubicin)liposome for injection versus conventional cytarabine plus daunorubicin in older patients with newly diagnosed secondary acute myeloid leukemia[J]. J Clin Oncol, 2018, 36(26): 2684-2692. doi: 10.1200/JCO.2017.77.6112
[19] Talati C, Goldberg AD, Przespolewski A, et al. Comparison of induction strategies and responses for acute myeloid leukemia patients after resistance to hypomethylating agents for antecedent myeloid malignancy[J]. Leuk Res, 2020, 93: 106367. doi: 10.1016/j.leukres.2020.106367
[20] Campos L, Rouault JP, Sabido O, et al. High expression of bcl-2 protein in acute myeloid leukemia cells is associated with poor response to chemotherapy[J]. Blood, 1993, 81(11): 3091-3096. doi: 10.1182/blood.V81.11.3091.3091
[21] Wang HF, Mao LP, Yang M, et al. Venetoclax plus 3+7 daunorubicin and cytarabine chemotherapy as first-line treatment for adults with acute myeloid leukaemia: a multicentre, single-arm, phase 2 trial[J]. Lancet Haematol, 2022, 9(6): e415-e424. doi: 10.1016/S2352-3026(22)00106-5
[22] Bataller A, Bazinet A, Borthakur G, et al. CPX-351 with venetoclax in patients with relapsed/refractory acute myeloid leukemia: results of a phase ib study[J]. Blood, 2023, 142: 4259. doi: 10.1182/blood-2023-181786
[23] Röllig C, Fransecky L, Hanoun M, et al. Venetoclax plus high-dose cytarabine and mitoxantrone As feasible and effective novel treatment for relapsed AML: results of the phase-Ⅰ SAL relax trial[J]. Blood, 2022, 140(Supplement 1): 3327-3328. doi: 10.1182/blood-2022-159897
[24] Pei SS, Shelton IT, Gillen AE, et al. A novel type of monocytic leukemia stem cell revealed by the clinical use of venetoclax-based therapy[J]. Cancer Discov, 2023, 13(9): 2032-2049. doi: 10.1158/2159-8290.CD-22-1297
[25] Hou Y, Dovat K, Dovat S, et al. Pb1784: cladribine synergizes the effect of venetoclax on cell proliferation arrest and apoptosis by targeting dna-pkcs/c-myc signaling in acute myeloid leukemia[J]. Hema Sphere, 2023, 7(S3): e94050b8.
-

计量
- 文章访问数: 350
- 施引文献: 0