
-
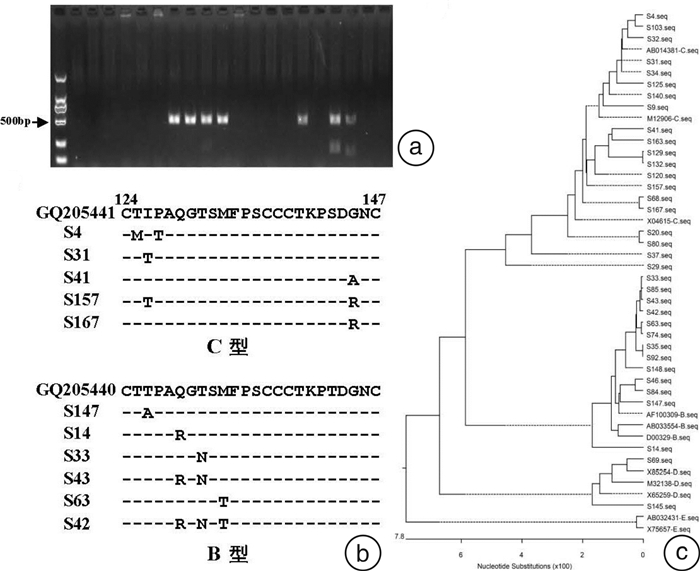
摘要: 目的 对献血者血液筛查HBV阳性样本进行深入分析,探讨献血者HBV筛查模式,以提高献血者HBV筛查的有效率,减少不必要的血液浪费。方法 收集165例经胶体金检测HBsAg阴性而HBsAg酶联免疫(ELISA)阳性和(或)HBV核酸检测阳性的血液样本,定量检测其HBV血清学标志物,进行HBV S区序列分析。结果 2种ELISA试剂检测为阳性的样本共73例(44.24%),抗-HBc抗体阳性率为90.41%,HBsAg定量检测阳性率为75.34%;仅1种ELISA试剂检测为阳性的样本共68例(41.21%),抗-HBc抗体阳性率为26.47%,HBsAg定量检测阳性率为1.47%;HBsAg定量检测阳性样本中79.31%的HBsAg低于10 IU/mL; 共扩增出35例HBV S区片段,30例确定为HBV C型基因,5例确定为B型基因,未发现影响HBsAg检测的突变。结论 HBV病毒载量、HBsAg水平极低可导致HBV筛查假阴性,而单独1种ELISA试剂检测HBsAg存在较多假阳性结果。实验室可结合HBV检测方法及检测试剂的性能验证结果,制订适合自身的检测策略。Abstract: Objective To analyze the samples which were positive by blood screening for HBV of blood donors, improve the efficiency of blood donor screening and reduce unnecessary blood waste.Methods Totally 165 samples with non-reactive results by colloidal gold detection HBsAg but reactive results by HBsAg ELISA test and/or HBV NAT were collected. The serological markers for HBV infection were further quantitative assessed by chemiluminescentmicroparticle immunoassay(CLIA). The viral S regions were amplified by nested PCR and then analyzed.Results In total 73 samples(44.24%) were HBsAg reactive with two ELISA kits, in which 90.41% were positive for anti-HBc and 75.34% were positive for HBsAg quantitative detection. Totally 68 samples(41.21%) were just HBsAg reactive with one ELISA kits, in which the positive rate of anti-HBc and HBsAg quantitative detection were 26.47% and 1.47%, respectively. 79.31% of HBsAg quantitative positive samples were less than 10 IU / mL. A total of 35 cases of HBV S region were amplified, 30 cases were identified as HBV C gene, 5 cases were identified as HBV B gene, and no mutations that affected the detection of HBsAg were found.Conclusion The extremely low HBV DNA load and HBsAg titer were the cause of false negatives in the blood screening of blood donor. However, there would be many false positives in samples with a single ELISA kit reactive. Test strategy should be generated according to the results of performance verification of methods and reagents for HBV test.
-
Key words:
- hepatitis B virus /
- blood screening /
- blood donor
-

-
表 1 巢式PCR扩增HBV S区片段基因所用引物
序号 引物序列 第1轮 S-1stF 5′AGAACATCGCATCAGGACTC3′ S-1stR 5′CCCCACTGT(T/C)TGGCTTTCAG3′ 第2轮 S-2ndF 5′TCGTGTTACAGGCGGGGTTT3′ S-2ndR 5′CGAACCACTGAACAAATGGC3′  下载: 导出CSV
下载: 导出CSV
表 2 HBV血清学标志物定量检测结果
%(例/例) 结果 例数/例(%) HBsAg 抗-HBs阳性率 抗-HBe阳性率 抗-HBc阳性率 HBsAg阳性率 0.05~1.00 IU/mL 1.00~10.00 IU/mL 2ELISA+NAT+ 26(15.76) 96.15(25/26) 60.00(15/25) 28.00(7/25) 3.85(1/26) 80.77(21/26) 100(26/26) 2ELISA+NAT- 47(28.48) 63.83(30/47) 46.67(14/30) 23.33(7/30) 4.26(2/47) 78.72(37/47) 85.11(40/47) 1ELISA+NAT+ 3(1.82) 66.67(2/3) 100(2/2) 0 0 66.67(2/3) 100(3/3) 1ELISA+NAT- 68(41.21) 1.47(1/68) 100(1/1) 0 54.41(37/68) 11.76(8/68) 26.47(18/68) 2ELISA-NAT+ 21(12.73) 0 / / 19.05(4/21) 19.05(4/21) 76.19(16/21) 合计 165(100.00) 35.15(58/165) 55.17(32/58) 24.14(14/58) 26.67(44/165) 43.64(72/165) 62.42(103/165)
下载: 导出CSV
-
[1] Shi J. Status analysis and evaluation of the blood scrap rate from 2015-2017 for a blood center in China[J]. Transfus Clin Biol, 2020, 27(3): 109-114. doi: 10.1016/j.tracli.2020.06.010
[2] 冯瑾, 刘璇. 成都地区无偿献血者的职业分布及检测不合格情况调查[J]. 中国输血杂志, 2019, 32(4): 376-378. https://www.cnki.com.cn/Article/CJFDTOTAL-BLOO201904023.htm
[3] 王乐, 汪峰, 莫艳萍, 等. 无偿献血者血液HBsAg、抗-HCV、抗-HIV和抗-TP不合格情况分析及研究[J]. 临床血液学杂志, 2021, 34(4): 263-267. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXZ202104011.htm
[4] 中华医学会感染病学分会. 中华医学会肝病学分会. 慢性乙型肝炎防治指南(2019年版)[J]. 临床肝胆病杂志, 2019, 35(12): 2648-2669. https://www.cnki.com.cn/Article/CJFDTOTAL-LCGD201912010.htm
[5] 冯涛, 朱胜江, 朱绍汶, 等. 献血者HBsAg ELISA筛查单试剂假阳性的原因分析[J]. 中国实验血液学杂志, 2020, 28(4): 1386-1390. https://www.cnki.com.cn/Article/CJFDTOTAL-XYSY202004057.htm
[6] 庞栋, 申卫东, 张翙, 等. ELISA筛查单试剂反应献血者追踪检测[J]. 中国输血杂志, 2014, 27(4): 381-383. https://www.cnki.com.cn/Article/CJFDTOTAL-BLOO201404014.htm
[7] Ye X, Zhao Y, Li R, et al. High Frequency Occult Hepatitis B Virus Infection Detected in Non-Resolved Donations Suggests the Requirement of Anti-HBc Test in Blood Donors in Southern China[J]. Front Immunol, 2021, 12: 699217.
[8] Ye X, Li T, Li R, et al. Molecular characteristics of HBV infection among blood donors tested HBsAg reactive in a single ELISA test in southern China[J]. BMC Infect Dis, 2021, 21(1): 83. doi: 10.1186/s12879-020-05747-4
[9] Kuhns MC, Holzmayer V, Anderson M, et al. Molecular and Serological Characterization of Hepatitis B Virus(HBV)-Positive Samples with Very Low or Undetectable Levels of HBV Surface Antigen[J]. Viruses, 2021, 13(10): 2053. doi: 10.3390/v13102053
[10] Wang H, Wang M, Huang J, et al. Novel hepatitis B virus surface antigen mutations associated with occult genotype B hepatitis B virus infection affect HBsAg detection[J]. J Viral Hepat, 2020, 27(9): 915-921.
[11] Ye X, Li T, Shao W, et al. Nearly half of Ultrio plus NAT non-discriminated reactive blood donors were identified as occult HBV infection in South China[J]. BMC Infect Dis, 2019, 19(1): 574. doi: 10.1186/s12879-019-4215-9
[12] Tang Y, Liu X, Lu X, et al. Occult Hepatitis B Virus Infection in Maintenance Hemodialysis Patients: Prevalence and Mutations in "a" Determinant[J]. Int J Med Sci, 2020, 17(15): 2299-2305.
[13] Liu Y, Li P, Li C, et al. Detection of hepatitis B virus DNA among accepted blood donors in Nanjing, China[J]. Virol J, 2010, 7: 193.
[14] 何成涛, 庞蓉蓉, 马成平, 等. 2015—2017年血液筛查室间质评结果分析[J]. 临床血液学杂志, 2019, 32(8): 614-617. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXZ201908013.htm
-
图(1)
表(2)
计量
- 文章访问数: 662
- PDF下载数: 253
- 施引文献: 0